The transatlantic regulatory split between the U.S. Food and Drug Administration and the European Medicines Agency stopped being a compliance footnote sometime around 2021. It is now a capital allocation variable. A company that misreads the divergence between these two systems doesn’t just face delayed approvals — it faces compressed exclusivity windows, mispriced pipeline assets, and biosimilar exposure it didn’t model correctly.
This page maps the full architecture of the FDA-EMA divide: structural, legal, IP-linked, commercial, and financial. It is written for the people who use this information to make decisions — portfolio managers stress-testing LOE timelines, BD teams pricing licensing deals, IP counsel building Paragraph IV defense strategies, and commercial forecasters modeling biosimilar erosion curves. Every section targets a distinct decision-point or search intent. None of it is filler.
How the FDA and EMA Are Structurally Incompatible — and Why That Matters for Launch Sequencing
The FDA and EMA share a scientific mission. Operationally, they are different institutions running on different legal architectures, which means they produce different timelines, different data requirements, and different commercial outcomes.
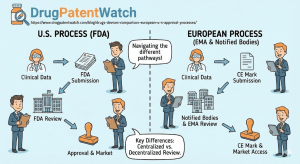
The FDA operates as a unitary federal agency under the Federal Food, Drug, and Cosmetic Act. Every NDA, BLA, and 510(k) is reviewed by federal employees inside CDER, CBER, or CDRH. When an approval letter is issued, the product is legal in all 50 states. No political ratification. No secondary conversion step. The approval is the approval.
The EMA is not an approval body in the same sense. It coordinates a network of over 4,500 scientific experts drawn from the 27 National Competent Authorities — Germany’s BfArM, France’s ANSM, the Netherlands’ CBG, Sweden’s MPA, and others. The CHMP issues a “positive opinion,” not an approval. That opinion then goes to the European Commission, which converts it into a legally binding Marketing Authorization in approximately 67 days. That administrative gap — baked into treaty architecture — is one of several structural reasons why U.S. approval consistently precedes EU authorization.
For a drug with a compound patent expiring in, say, 2031, that 67-day administrative gap isn’t trivial. It compresses the EU revenue window by two months before a single prescriber has written a script.
What the FDA’s PDUFA Structure Means for Predictability — and Why Investors Price It Differently
PDUFA — the Prescription Drug User Fee Act — does something structurally valuable for investors: it converts regulatory timelines into contractual commitments. Industry fees fund the FDA’s review capacity, and in exchange, the FDA commits to reviewing standard applications within 10 months and priority applications within 6. These deadlines are tracked, reported on annually, and historically met at high rates.
The EMA’s 210-day “active review” clock sounds comparable but operates differently. The clock excludes “clock stops” — periods where the review is paused while the sponsor responds to Day 120 or Day 180 questions. A typical MAA with one or two clock stops runs 12 to 15 calendar months. That’s not a worst-case scenario; it’s the median.
For a product priced at $5,000 per month, three extra months of EU regulatory delay is roughly $15,000 in lost revenue per patient who switches to a competitor during the wait. At 50,000 patients, that’s $750 million.
Why the European Commission’s 67-Day Conversion Step Creates a Structural LOE Disadvantage
The EC conversion step is easily overlooked because it almost never fails — the Commission has rejected a CHMP positive opinion fewer than five times in the agency’s history. But the calendar lag is real, and it stacks on top of HTA timelines, pricing negotiations, and national formulary listings. A drug approved by the FDA in January 2025 might not be reimbursed in France until late 2026. In that window, competing mechanisms or biosimilars may already be establishing market share.
Table 1: Structural Authority Comparison
Feature
FDA
EMA
Legal Basis
FD&C Act
Regulation (EC) 726/2004 + Directive 2001/83/EC
Jurisdiction
USA (single federal market)
27 Member States + EEA
Reviewer Type
Federal employees (centralized)
National experts (networked)
Final Decision Holder
FDA Commissioner (delegated)
European Commission (political body)
Calendar-to-Approval
~10 months standard, ~6 months priority
~12-15 months including EC step
Device Regulation
CDRH (within FDA)
Notified Bodies (private, accredited)
Pricing Authority
None (IRA negotiations beginning 2026)
None (delegated to Member States)
Why 68% of Novel Drugs Launch in the U.S. First — and What That Means for Patent Clock Economics
In 2024, the FDA’s CDER approved 50 novel drugs; the EMA authorized 46 new active substances. The raw counts look similar. The timing does not. According to Citeline analysis, the FDA held an overwhelming lead in first-launch position for novel drugs, with U.S. approval preceding European authorization in the majority of cases across oncology, neurology, and rare disease.
The economics of first-launch position compound over the life of a product. A drug that launches in the U.S. six months before Europe generates U.S. revenue while European HTA clock starts ticking — meaning the sponsor can use that commercial runway to fund the market access arguments in Germany, France, and England. A drug that enters Europe first (rare, but it happens) often does so in smaller indications where U.S. trial design wasn’t yet mature enough for an NDA.
How Accelerated Approval Widens the U.S.-EU Oncology Gap
The FDA’s Accelerated Approval pathway — codified under 21 CFR § 601.41 — allows approval based on surrogate endpoints “reasonably likely to predict” clinical benefit. Tumor shrinkage rate, progression-free survival, and MRD negativity in hematologic malignancies have all served as accelerating endpoints. The confirmatory trial comes post-approval.
The EMA’s analog, Conditional Marketing Authorization (CMA), requires more. Sponsors generally need to demonstrate that the benefit-risk balance is positive even on incomplete data, and the “reasonable likelihood” standard in the EU is interpreted more conservatively than in the U.S. The EMA also tends to require a clear path to converting the CMA to a standard authorization within a defined timeline — typically 12 to 24 months.
The practical consequence: a first-in-class IO combination or ADC entering a solid tumor indication will almost always receive FDA Accelerated Approval before CMA. From 2019 to 2024, FDA approved 199 solid tumor indications; EMA approved the same indications a median of 181 days later. That gap has remained structurally consistent for a decade.
Kisunla and Leqembi: The Alzheimer’s Case Study in Regulatory Philosophy
The divergence in Alzheimer’s approvals illustrates a deeper philosophical split. Eli Lilly’s Kisunla (donanemab) received FDA approval in July 2024 based on amyloid clearance and slowing of cognitive decline on the integrated Alzheimer’s Disease Rating Scale. The EMA was still reviewing the file at year-end.
Biogen and Eisai’s Leqembi (lecanemab) followed a similar arc — FDA approval well ahead of EMA, with the EU authorization arriving more than a year later. Both drugs operate via amyloid beta plaque clearance, a mechanism the FDA accepted as “reasonably likely to predict” benefit; the EMA took longer to reach the same conclusion while weighing ARIA (amyloid-related imaging abnormalities) risk more conservatively.
For Lilly and Biogen/Eisai shareholders, that timeline gap translated directly into U.S. revenue without European competition, and to a longer U.S.-exclusive pricing window before parallel import dynamics could complicate things.
How the Hatch-Waxman Patent Linkage System Creates Structural Generic Delay — and Why the EU Deliberately Avoided It
This is the section that separates pharmaceutical IP strategy from regulatory compliance. The U.S. Hatch-Waxman Act created a system where FDA approval of a generic drug is legally tethered to the patent status of the originator. The EU made a deliberate choice not to replicate it.
Orange Book Listing Strategy: What Gets Listed and Why It Matters for Paragraph IV Exposure
The FDA’s Orange Book — formally, Approved Drug Products with Therapeutic Equivalence Evaluations — requires NDA holders to list patents covering the drug substance (active ingredient), the drug product (formulation), and methods of use. What’s conspicuously absent from that list: process patents, metabolite patents, and intermediate patents.
The listing decision is itself a strategic choice. A patent listed in the Orange Book becomes a Paragraph IV target; a patent not listed doesn’t trigger the automatic 30-month stay, but it still has value in post-ANDA-approval litigation. Companies making Orange Book listing decisions are simultaneously trying to maximize the barrier to ANDA entry while not listing patents that are so easy to design around that a Paragraph IV challenge attracts a generic filer and triggers litigation the originator might lose.
The 30-month stay is the centerpiece of the system. When a generic files an ANDA with a Paragraph IV certification — asserting that a listed patent is either invalid or won’t be infringed by the generic — and the NDA holder sues within 45 days, FDA approval of the generic is automatically stayed for 30 months from the date of the generic’s ANDA acceptance. The originator wins time regardless of whether the underlying patent holds up.
How Paragraph IV Certification Timing Determines When Generics Actually Enter the Market
The first ANDA filer with a successful Paragraph IV certification earns 180-day exclusivity — a period during which FDA cannot approve any other ANDA for the same drug. This exclusivity is commercially significant. A generic that captures a high-spend small molecule with 180-day exclusivity may face only one competitor for six months, allowing pricing at 70-80% of brand WAC rather than the 10-20% that comes later when seven or eight generics are on market.
For originators, the 180-day exclusivity creates an incentive structure where settling with the first filer is often commercially rational. A “reverse payment settlement” — where the originator pays the generic to delay launch — was limited by the Supreme Court’s 2013 FTC v. Actavis decision, which held that such payments can violate antitrust law if large enough. Post-Actavis, settlements shifted toward entering the market at a specific date (often at patent expiry or close to it) with a license, rather than pure cash payments.
Why the EU’s Lack of Patent Linkage Creates Different Generic Entry Dynamics
The EMA has no Orange Book, no Paragraph IV mechanism, and no automatic 30-month stay. A generic company can receive a Marketing Authorization from the EMA even while a valid SPC is in force. The authorization is simply held in abeyance until IP protection expires. Launching before expiry puts the generic “at risk” of national patent infringement suits — but those suits are litigated in national courts (Germany, UK, France, Netherlands) under national patent law, not federal law, and outcomes vary.
This structure shifts leverage toward generics in certain scenarios. In Germany, for instance, preliminary injunctions in pharmaceutical patent cases are granted more readily than in some other jurisdictions, effectively creating a quasi-linkage effect through litigation risk even without statutory patent linkage. In the Netherlands, cross-border injunctions through the Dutch courts have been used to block pan-European generic launches during SPC protection.
The absence of federal linkage means EU generic exposure timelines are harder to model than U.S. ones. There’s no public “trigger” notification when a generic files for EU authorization. Companies must actively monitor European Patent Office SPC filings, national court dockets, and EMA authorization databases — a monitoring challenge that intelligence platforms like DrugPatentWatch aggregate from disparate sources.
SPC Duration Mechanics: What the 5-Year Extension Actually Covers
Supplementary Protection Certificates extend patent protection for up to five years (plus an additional six months for pediatric studies) to compensate for time lost during regulatory review. The duration formula is: date of first EU authorization minus date of patent filing, minus five years, capped at five years maximum. A product that took 12 years from patent to authorization gets a 5-year SPC; one that took 8 years gets a 3-year SPC.
The critical distinction from U.S. Patent Term Extension: SPCs are granted at the national level, not EU-wide. A drug might lose SPC protection in France two months before Germany because the German SPC was filed on a different patent. This creates a fragmented exclusivity cliff where generics can enter one country while protection remains in another — useful for originators who can reprice selectively in earlier-expiry markets.
Table 2: U.S. vs. EU IP Exclusivity Mechanisms
Mechanism
U.S.
EU
Patent term
20 years from filing
20 years from filing
Patent term extension
PTE: up to 5 years (Hatch-Waxman § 156)
SPC: up to 5 years nationally
Pediatric extension
6 months (BPCA)
6 months (EU Pediatric Regulation)
Generic entry trigger
Paragraph IV ANDA + lawsuit = 30-month stay
No linkage; generic MAs can be granted during SPC
Data exclusivity (NCE)
5 years
8 years
Market exclusivity (NCE)
3 additional years for new clinical investigation
2 additional years
Biologic exclusivity
12 years data; no automatic biosimilar stay
8 years data; 2 years market
Orphan exclusivity
7 years
10 years
First generic exclusivity
180 days (Paragraph IV filer)
None at federal level
Why the EU Pharmaceutical Legislation Revision Threatens the 8+2+1 Exclusivity Framework
The European Commission’s proposed revision to EU pharmaceutical legislation, under active legislative debate since 2023, includes a proposal to reduce baseline data exclusivity from 8 years to 6 years for NCEs unless certain conditions are met — primarily, launching in all EU Member States within two years of authorization.
This “launch obligation” mechanism has drawn sharp criticism from EFPIA, which modeled the impact at a loss of approximately 15-20 NMEs per decade for European patients due to reduced R&D investment incentives. The pharmaceutical industry’s position is that reducing exclusivity while simultaneously adding the JCA burden and compressing AMNOG free-pricing windows makes Europe materially less attractive for first-in-class launches.
Generics and biosimilar manufacturers, represented by Medicines for Europe, argued the opposite: that the current framework overprotects originators and delays patient access to affordable medicines. The legislative outcome will define the commercial calculus for drugs entering development today, given typical 10-12 year development timelines.
For companies currently in Phase II with assets targeting EU launch in 2030-2033, the exclusivity uncertainty is a real risk to NPV modeling. Products designed around an 8-year data exclusivity assumption may see that assumption legislated away before commercialization.
What the EU MDR Has Done to Medtech’s First-Launch Geography — and Why It’s Worse Than the Drug Side
If the drug gap is a competitive disadvantage, the medical device divergence is a structural exodus. The EU Medical Device Regulation (MDR), fully applicable since May 2021, has driven a measurable shift in medtech first-launch geography. The instrument meant to strengthen European device oversight has instead hollowed out the EU’s competitive position as an innovation market.
How the MDR Notified Body Bottleneck Created a 24-Month Approval Crisis
Under the old Medical Device Directive (MDD), approximately 80+ Notified Bodies operated across the EU to audit and certify devices. MDR’s tighter requirements — including auditor qualifications, unannounced inspections, and clinical evidence standards — triggered a wave of Notified Body exits. The number of designated bodies capable of reviewing MDR applications fell dramatically in the years following MDR application. Capacity contracted just as the certification workload tripled from mandatory legacy device recertification.
The arithmetic is predictable: MedTech Europe’s 2024 survey found a 33% decline in large manufacturers choosing the EU as their first-launch geography for devices. Companies that once launched in Europe first to generate revenue and real-world data for the FDA PMA process are now reversing the sequence. The FDA’s 510(k) pathway for Class II devices takes 3-6 months at a cost of roughly $20,000 in user fees. MDR certification for a comparable device now takes 18-24 months and can cost $500,000 to $2 million in Notified Body fees, clinical data generation, and Quality Management System upgrades.
Why 510(k) Substantial Equivalence Remains the Most Commercially Efficient Device Pathway Globally
The 510(k)’s core mechanism — demonstrating substantial equivalence to a legally marketed predicate device — requires no clinical trial data for most Class II applications. A company with a new orthopedic implant, a drug-eluting stent iteration, or a continuous glucose monitor upgrade can typically identify a predicate, build the technical file, pay the user fee, and be cleared within six months.
MDR’s version of equivalence is structurally different. To claim equivalence to a competitor device, the applicant must have access to the competitor’s technical documentation — which competitors are not obligated to share. In practice, equivalence claims are only viable for devices with the same corporate lineage (product revisions from the same manufacturer). Everything else requires a new clinical investigation under MEDDEV 2.7/1 rev. 4 criteria.
That’s not a minor procedural hurdle. For a Class IIb implant, a new EU clinical investigation might require a 200-300 patient randomized controlled trial with 24-month follow-up before CE marking is granted. The same product might already be on the U.S. market two years before European patients have access.
The Orphan Device Problem: What Happens When MDR Compliance Exceeds Product Revenue
The crisis is most acute for devices treating rare conditions or pediatric populations. A device indicated for a condition affecting 10,000 patients in the EU generates limited revenue. MDR compliance for that device — recertification costs, PMCF study requirements, EUDAMED registration, QMS upgrades — can exceed five years of EU product revenue. Manufacturers are choosing to withdraw. CE marks that were valid for decades are not being renewed because the economics no longer support recertification.
The FDA’s Humanitarian Device Exemption provides a regulatory off-ramp for devices treating fewer than 8,000 U.S. patients per year, requiring only safety demonstration (not efficacy) with streamlined review and $6,375 in user fees. Europe has no equivalent valve. The result: patients with certain rare conditions now have access to devices in the U.S. that are simply unavailable in the EU because no manufacturer will absorb MDR compliance costs for a product that serves 1,000 European patients.
How the EU Clinical Trials Regulation Transition Created a Research Infrastructure Crisis
Clinical trial starts are the leading indicator of future drug approvals. A decline in European trial activity today means fewer EU-originated NMEs competing for global launch slots in 2030-2035. The CTR transition has been a significant headwind.
Why the CTIS Transition Deadline Concentrated Risk Into a Single Administrative Chokepoint
The Clinical Trials Regulation, fully applicable since January 2022, was designed to replace the patchwork of national applications under the Clinical Trials Directive with a single submission via the Clinical Trials Information System (CTIS). Every ongoing trial approved under the old Directive had to transition to CTIS by January 31, 2025.
By late 2024, a backlog of transition applications had created processing delays. Smaller biotechs and academic sponsors, many running Phase I/II programs for rare disease or oncology indications, found CTIS technically complex. Some sites flagged risk that ongoing trials might face a compliance gap if transition applications weren’t processed before the deadline. The EMA and Member States pushed communication campaigns, but the structural problem remained: a mandatory hard deadline for thousands of trial transitions converged on a system that had known capacity constraints from the day it launched.
Early-phase trial starts in Europe declined relative to the U.S. and Australia during this period. Some oncology sponsors moved Phase I dose-escalation studies to Australia — which allows commercial manufacturing experience to transfer to TGA submissions and, via Project Orbis, potentially to the FDA — specifically to avoid European CTR friction during the transition window.
How the IND 30-Day Passive Approval Mechanism Structurally Advantages U.S. Trial Initiation
The U.S. Investigational New Drug application operates on passive approval logic. Submit the IND. If the FDA does not place the trial on clinical hold within 30 days, proceed. For most first-in-human studies with reasonable safety packages, this means a 30-day clock from submission to first patient enrollment eligibility.
EU CTR requires active authorization. Each participating Member State reviews the application through CTIS. Timelines vary by country and by how questions are coordinated across national competent authorities and ethics committees. For a multi-country EU trial, the authorization process routinely takes three to four months for straightforward protocols and longer for complex designs.
The cumulative effect: a U.S. company with an IND-ready package can initiate U.S. trials one to two quarters before comparable EU sites are authorized. That advantage compounds when U.S. data is used to support an EU CMA dossier — the U.S. trial completes while EU trials are still enrolling.
Why the Inflation Reduction Act Changes Every LOE Calculation for Drugs Launching After 2022
The Inflation Reduction Act’s drug pricing provisions represent the largest structural change to U.S. pharmaceutical economics since Hatch-Waxman. For pipeline assets currently in Phase III, the IRA effectively resets the NPV model.
How IRA Price Negotiations Work — and Which Drug Types Face the Highest Exposure
The IRA allows CMS to “negotiate” (in practice, to mandate) prices for Medicare Part B and Part D drugs that meet defined criteria. In the first round, the 10 highest-spend Part D drugs without generic or biosimilar competition were selected. Published prices for drugs including apixaban (Eliquis, Bristol Myers Squibb/Pfizer) and empagliflozin (Jardiance, Boehringer Ingelheim/Eli Lilly) reflected minimum 38% reductions from list price for Medicare, effective January 2026.
The negotiation trigger timeline: small molecules become eligible 9 years after first approval; biologics at 13 years. Small molecules face an earlier cliff because the shorter exclusivity window (9 vs. 13 years) means more products become eligible sooner. This creates a structural incentive to develop biologics over small molecules for certain therapeutic areas where both modalities are viable, or to invest in biologics manufacturing capabilities that support 13-year protection.
What IRA Orphan Drug Exemption Loss Means for Rare Disease Lifecycle Management
A drug approved solely for one rare disease is exempt from IRA negotiation. This exemption disappears if the drug receives a second approval — for a different rare disease or for a common indication. The implication for lifecycle management is direct: the multi-indication strategy that once maximized asset value (approve for rare disease first, expand to broader indications) now carries a tax in the form of IRA negotiation eligibility.
A drug approved for one orphan indication generating $2 billion annually in Medicare spend might remain exempt indefinitely. The same drug approved for a second indication — even another rare disease — enters the negotiation pool at year 9 (small molecule) or year 13 (biologic). The revenue from the second indication may be smaller than the revenue concession from IRA-negotiated pricing on the first.
How U.S.-EU Price Differentials Are Narrowing — and What That Means for Global Pricing Strategy
Historically, U.S. list prices ran 3 to 9 times European reimbursed prices. IRA negotiated prices will narrow that gap for high-spend Medicare drugs, but net prices in the U.S. remain substantially above European levels. More importantly, IRA negotiation affects Medicare prices only — commercial insurance pricing remains unaffected, and commercial represents the majority of revenue for most brands.
The pricing-pressure narrative overstates the near-term IRA impact. The longer-term risk is that IRA creates a precedent that expands. If Congress extends the IRA negotiation framework to commercial insurance prices, the calculus changes completely. That expansion is not current law, but it is a scenario that financial models for assets with 2030+ LOE dates should stress-test.
How the EU Joint Clinical Assessment Creates a Fourth Hurdle — and Which Therapeutic Areas Face the Most Risk
The EU HTA Regulation, implemented January 2025 for oncology and ATMPs, created a new Joint Clinical Assessment (JCA) process that runs in parallel with EMA review. The JCA is supposed to harmonize the clinical evidence assessments that formerly happened separately in Germany, France, England, Spain, and 23 other countries. In practice, it may add a layer of risk that national HTAs did not.
Why the PICO Scoping Problem Could Sink Market Access Despite EMA Approval
The JCA’s output is a relative effectiveness assessment comparing the new drug to a defined comparator — the Comparator arm of the PICO (Population, Intervention, Comparator, Outcome) framework. The comparator is determined during a PICO scoping exercise that happens before the clinical data is reviewed.
The risk: the EU PICO scoping committee might define the comparator differently than the comparator used in the pivotal clinical trial. A drug trialed against placebo (because no active comparator existed at trial design) might be assessed against a standard-of-care that emerged during the trial period. If the JCA’s PICO-defined comparator doesn’t match the trial design, the relative effectiveness assessment may be inconclusive or negative — not because the drug doesn’t work, but because the trial wasn’t designed to answer the JCA’s specific question.
A negative or inconclusive JCA report doesn’t block reimbursement — Member States retain that authority — but it creates a problematic starting point for national HTA bodies. Germany’s GBA, France’s HAS, and England’s NICE will all receive the JCA report as context for their national assessments. A JCA conclusion that “relative effectiveness versus the EU standard-of-care comparator could not be determined” gives national payers cover to delay, discount, or reject reimbursement applications.
Why Germany’s AMNOG Free-Pricing Window Matters More Than Most Reimbursement Models Account For
Under the AMNOG framework, drugs launched in Germany can be sold at the list price for the first 12 months before a negotiated price takes effect. This “free pricing period” was a primary reason Germany served as the standard EU first-launch market — a company could generate 12 months of near-U.S. list price revenue while European HTA processes ran.
That window has been compressed to 6 months. A drug launching in Germany in Q1 2026 must have its AMNOG dossier submitted at launch and will face negotiated pricing by Q3 2026. For high-priced drugs, the six-month truncation of free pricing can reduce German revenue by tens to hundreds of millions of euros over product lifecycle — a direct NPV impact.
Why Project Orbis Proves the FDA Can Build Alliances the EMA Cannot
Project Orbis is the FDA’s oncology concurrent-review initiative, operating with partners including Australia’s TGA, Canada’s Health Canada, the UK’s MHRA, Switzerland’s Swissmedic, Brazil’s ANVISA, Singapore’s HSA, and Israel’s Ministry of Health. Applications are submitted in parallel; reviews proceed simultaneously; approvals can be issued within weeks of each other across all participating jurisdictions.
The EMA participates as an observer only. It cannot legally join as a full participant because the EU Centralized Procedure operates on treaty-defined timelines and requires the consensus of 27 national representatives — a process that cannot synchronize with the real-time data exchange and rolling-review mechanics of Orbis.
The consequence for patients is measurable. An oncology drug approved through Project Orbis receives market access in seven to eight countries within a compressed window. EU patients wait months to years longer. The UK, now outside the EU post-Brexit, is a full Orbis participant — meaning British patients with cancer may access new therapies before French or German patients, despite the UK and EU both being wealthy European markets with sophisticated healthcare infrastructure.
For commercial forecasters, this means modeling Project Orbis countries as a distinct revenue cluster with different launch timing, pricing dynamics, and market access profiles than the EU.
How Biosimilar Interchangeability Designation Functions Differently in the U.S. and EU — and Why It Determines Revenue Erosion Speed
The rate of revenue erosion after loss of exclusivity depends heavily on whether biosimilars can be substituted automatically at the pharmacy level. This is where the U.S. interchangeability designation becomes commercially significant — and where the EU’s patchwork substitution framework creates unpredictable market dynamics.
What FDA Interchangeable Biosimilar Designation Requires — and Which Products Have Achieved It
Under Section 351(k) of the Public Health Service Act, a biosimilar can receive “interchangeable” designation if it meets biosimilarity criteria and demonstrates, via switching studies, that alternating between the biosimilar and the reference product produces no greater safety or efficacy risk than continued use of the reference product. Interchangeable products can be substituted by pharmacists without prescriber authorization, subject to individual state laws.
As of 2024, multiple biosimilars to adalimumab (Humira, AbbVie), insulin analogs, and pegfilgrastim had received interchangeable designation. Achieving interchangeability requires two to three switching studies, typically adding six to twelve months and several million dollars to biosimilar development costs. The commercial payoff is direct: an interchangeable designation on a high-volume biologic means pharmacy-level substitution drives volume without requiring sales force detailing of each prescriber.
How the EU Handles Biosimilar Substitution Without an Interchangeability Designation
The EMA has no statutory interchangeability designation. Instead, EMA and the Heads of Medicines Agencies published guidance stating that EU-approved biosimilars are scientifically appropriate for interchangeability decisions, while deferring the actual substitution policy to Member States.
France allows pharmacist substitution for biosimilars on a designated list. Italy allows it for new patients. Germany does not allow substitution at the pharmacy level, though the GKV-Spitzenverband can mandate biosimilar quotas through tendering. The Netherlands and Belgium have moved toward active substitution policies. The UK post-Brexit is implementing its own framework.
The result is that biosimilar penetration in the EU varies radically by country, product, and policy cycle — far more variable than the U.S., where interchangeability designation creates a more uniform commercial playbook.
What the ‘Rebate Wall’ Looks Like in Practice — and Whether IRA Is Dismantling It
In the U.S., originator companies have maintained formulary position for biologics like adalimumab by offering insurers and PBMs substantial rebates — sometimes 40-60% off list price — in exchange for preferred placement over biosimilars. A biosimilar that enters at 30% below list price may still cost the payer more on net if the originator’s rebate exceeds the biosimilar’s nominal discount.
This dynamic slowed biosimilar uptake for the first several years after Humira biosimilar launches in 2023. By 2024, the picture began shifting. Multiple biosimilars on formulary, PBM pressure, and growing employer pushback on branded rebate structures have started eroding AbbVie’s formulary defenses. CVS and Express Scripts both moved biosimilar adalimumab to preferred tier for certain employer books.
IRA accelerates this transition indirectly. As drug pricing transparency increases and payer sensitivity to biologics spend rises, the incentive to maintain a rebate wall weakens. The commercial case for biosimilar switching strengthens in a post-IRA pricing environment where every line-item biologic expenditure is scrutinized.
How SPC Manufacturing Waiver Mechanics Give EU Generics a Stockpiling Advantage
A regulatory mechanism with no U.S. equivalent — the EU SPC Manufacturing Waiver, in force since 2019 — allows EU-based generic and biosimilar manufacturers to produce product during the SPC protection period for two purposes: export to countries where the SPC has already expired, and stockpiling during the final six months of SPC protection to prepare for “Day 1” EU launch.
This matters commercially for biosimilars of large biologics. Manufacturing scale-up for a biosimilar monoclonal antibody requires 12 to 18 months of production cycles before commercial quantities are available. Without stockpiling capability, a biosimilar developer must start the launch clock with empty warehouses and supply patients from ongoing production. The SPC Manufacturing Waiver allows EU manufacturers to build six months of safety stock before the SPC expires, enabling an immediate commercial launch on Day 1.
U.S. law has a Bolar exemption covering R&D activity during patent term, but it does not extend to commercial stockpiling. U.S. biosimilar developers must manage the ramp-up risk without pre-expiry inventory buildup. For highly complex biologics with long batch cycle times, this creates meaningful supply risk in the first weeks after LOE.
How Post-Market Surveillance Requirements Under MDR and FDA Differ — and What It Costs
Why EU MDR’s Post-Market Clinical Follow-up Is an Ongoing Cost Center, Not a One-Time Event
The MDR requires manufacturers to actively collect clinical data on their devices for the entire commercial lifetime of the product — “Post-Market Clinical Follow-up.” This is not passive adverse event reporting. It requires structured PMCF plans, periodic PMCF evaluation reports, and in many cases, active registries or post-market clinical investigations.
For a high-volume implant like a total knee replacement system with hundreds of thousands of implants globally, maintaining a PMCF registry with minimum five-year clinical follow-up data means funding a clinical infrastructure indefinitely. For a software-as-a-medical-device (SaMD) product with annual software updates, determining what constitutes a “significant change” requiring new PMCF evaluation adds regulatory complexity to the product development cycle.
The FDA’s post-market obligations for Class II devices cleared via 510(k) are primarily passive — MDRs (Medical Device Reports) filed when malfunctions or serious adverse events occur, plus any conditions imposed through the clearance letter. Active post-market studies are required for some PMA devices but are product-specific, not universally mandated by device class.
REMS vs. RMP: What Institutional Investors Miss About Post-Market Drug Risk
The FDA’s REMS program applies to specific products where the agency has determined that standard labeling is insufficient to ensure safe use. REMS requirements vary: some are limited to a Medication Guide; others include ETASU (Elements to Assure Safe Use) requiring prescriber certification, patient enrollment in registries, and dispensing only through certified pharmacies.
Products with REMS have narrower patient access by design. For a prescriber not enrolled in the certification program, the drug is simply unavailable. From an investor perspective, REMS drugs carry lower addressable market than their clinical profile might suggest, and REMS modifications — either adding or removing requirements — can materially affect commercial execution.
The EMA’s Risk Management Plan is mandatory for every new medicine. Unlike REMS, it covers the entire product rather than specific safety concerns. RMPs are publicly summarized and updated throughout product life. The EMA’s EURD list (list of Union references dates) triggers periodic safety update report submissions that are coordinated across all EU member states — a surveillance architecture that creates more standardized pharmacovigilance data than the fragmented state-level reporting that characterizes much of U.S. device vigilance.
Key Patent Expiry Dates and LOE Events Investors Should Track Through 2030
Loss of exclusivity events are the primary driver of pharma revenue volatility. The following represent significant upcoming LOE inflection points across key products, with both U.S. and EU dimensions to track.
Keytruda (pembrolizumab, Merck): Core composition patents expire in 2028 in key markets. Merck has filed extensive method-of-use and formulation patents to extend protection. Biosimilar developers including Samsung Bioepis, Celltrion, and Alvotech have filed for biosimilar approval; the 12-year biologic data exclusivity in the U.S. provides protection until 2026 at the earliest from a regulatory pathway standpoint. Revenue exposure is approximately $25 billion annually.
Opdivo (nivolumab, Bristol Myers Squibb): Composition patents began expiring in major markets from 2026; BMS has built a patent thicket around formulation, dosing, and combination therapy patents. European SPC protection runs differently than U.S. PTE. Biosimilar filings are active.
Ozempic and Wegovy (semaglutide, Novo Nordisk): Composition of matter patents on GLP-1 receptor agonists and the semaglutide molecule itself are being actively litigated. The core semaglutide patent expires in 2026 in some jurisdictions; extended-release formulation patents run later. Manufacturing complexity — requiring specialized peptide synthesis and extended lipophilic acylation chemistry — creates a practical barrier that outlasts formal patent protection.
Dupixent (dupilumab, Sanofi/Regeneron): Biologics data exclusivity and patent protection extend through the mid-2030s in the U.S. European SPC situations vary by country.
Entresto (sacubitril/valsartan, Novartis): A small-molecule combination product with a more predictable Hatch-Waxman exposure profile. Generic challenges have been filed; the Paragraph IV landscape is active.
Why GLP-1 Manufacturing Complexity Is a Moat That Survives Patent Expiry
Semaglutide’s composition patents are not the only barrier protecting Novo Nordisk and Eli Lilly from generic semaglutide and tirzepatide competition. The manufacturing process itself functions as a moat that has no legal expiry date.
What Makes Peptide GLP-1 Manufacturing Difficult for Generic Entrants
Semaglutide is a 31-amino-acid peptide with a C18 fatty diacid chain attached via a glutamic acid linker to lysine at position 26. Solid-phase peptide synthesis (SPPS) produces the peptide backbone; the acylation chemistry attaches the fatty acid chain. The final product must meet a purity specification stringent enough that even minor synthesis impurities can produce immunogenicity or reduced efficacy.
Generic peptide manufacturers exist — several Indian and Chinese API producers have peptide synthesis capacity. But the specific equipment, validated processes, and regulatory filing infrastructure required for semaglutide at commercial scale represent multi-year investment even after patents expire. The FDA’s scale-up and manufacturing requirements for ANDAs covering peptide drugs are significant. The FDA’s draft guidance on complex drug substances indicates that applicants must demonstrate that their manufacturing process produces a product with the same impurity profile as the reference, not just the same primary sequence.
Tirzepatide (Mounjaro/Zepbound, Eli Lilly) adds additional complexity — it is a dual GIP/GLP-1 receptor agonist, a longer peptide, and the acylation chemistry is more complex than semaglutide. Even if Lilly’s composition patents were invalidated tomorrow, meaningful generic competition would require three to five years of manufacturing development.
What Investors Are Watching: Key Financial Metrics Tied to Regulatory Outcomes
For institutional investors in pharmaceutical and biotech equities, regulatory events are binary catalysts that require understanding the underlying mechanism — not just the headline. The following metrics are the ones that matter most.
PDUFA date as a binary catalyst: FDA PDUFA dates are the clearest catalyst event in pharmaceutical investing. Miss rates are low (historically under 5% for standard reviews, somewhat higher for priority reviews with complex clinical questions). The key variable is not whether approval happens, but whether any post-approval REMS requirements or label restrictions narrow the addressable population.
30-month stay expiry: When Paragraph IV litigation resolves — either through settlement, court decision, or stay expiry without final judgment — the generic entry date becomes predictable. Models should account for the possibility of multiple ANDA filers achieving Paragraph IV certification in sequence.
EU PICO scoping outcome: For EU-focused launches, the JCA PICO scoping document is now a material regulatory event. A PICO that specifies a comparator the pivotal trial didn’t use signals difficult national HTA negotiations ahead.
SPC expiry in Germany: German SPC expiry is the event that triggers Day 1 generic competition in the EU’s largest pharmaceutical market by spend. Monitoring SPC expiry at the national registry level (DPMA for Germany) gives earlier warning than EU-level patent databases.
IRA negotiation list announcement: CMS announces the next cohort of IRA price negotiation candidates annually. A drug appearing on that list faces defined price reductions effective two years after selection. For drugs already on market and spending-eligible, the IRA negotiation announcement functions like a scheduled LOE event.
Which Competitors Benefit Most from FDA-EMA Approval Timeline Gaps
Biosimilar developers targeting Keytruda: The later the FDA makes its first biosimilar pembrolizumab approval official, the longer Samsung Bioepis, Celltrion, and others can rely on the U.S. exclusivity window to justify continued manufacturing investment.
EU-based generic manufacturers: The SPC Manufacturing Waiver gives EU-domiciled manufacturers a structural advantage on Day 1 biosimilar launches. Companies like Stada, Sandoz (now independent), and Hikma have invested in pre-expiry stockpiling capacity for European LOE events.
510(k) clearance specialists in medtech: Companies built around the U.S. 510(k) pathway — Invacare, Integra LifeSciences, Merit Medical — have a structural cost advantage in the current environment compared to EU-first strategies.
MHRA-reliant UK launches: Post-Brexit, the UK MHRA has operated its own approval pathway with significantly reduced EMA dependence. Several oncology drugs have received MHRA approval ahead of EMA authorization. UK pharma companies and companies with strong UK commercial infrastructure benefit disproportionately from being a Project Orbis member.
Common Investor Questions
Does a faster FDA approval always mean higher revenue? Not necessarily. FDA approval speed is necessary but insufficient. A drug approved in six months under Priority Review but launching into a crowded class without differentiated pricing will underperform a drug approved in ten months with Breakthrough Therapy Designation support for a first-in-class mechanism. The label language, REMS conditions, and companion diagnostic requirements that come out of the FDA review process often matter more than the absolute approval timeline.
Is the EU’s 8+2+1 framework actually at risk in the legislative revision? Yes. The European Commission’s proposal to reduce baseline data exclusivity from 8 to 6 years conditioned on universal EU launch is real and being negotiated through the EU legislative process. Current industry models for products with expected EU launches in 2028-2030 should scenario-plan around both outcomes.
How does Project Orbis affect ex-U.S. revenue modeling for oncology drugs? Significantly. A drug in Project Orbis can model near-simultaneous launches across the U.S., UK, Canada, Australia, Switzerland, and Singapore. That’s roughly 15% of global pharmaceutical spend available within months of U.S. approval, compared to the typical 18-30 month lag for those markets before Orbis.
What’s the practical timeline for a GLP-1 biosimilar to reach U.S. pharmacy shelves after semaglutide patent expiry? Even assuming the composition patents expire on schedule, the manufacturing scale-up, ANDA preparation, FDA review, and commercial distribution infrastructure build-out suggests 3-5 years from patent expiry before meaningful market share for any single biosimilar semaglutide product.
Does MDR compliance affect a device company’s U.S. IPO valuation? It appears to. Several medtech companies with heavy EU revenue exposure have faced investor scrutiny about MDR recertification timelines and costs during U.S. IPO processes from 2022-2024. A device company with 40% EU revenue and a portfolio of legacy devices requiring MDR recertification by 2027 carries real off-balance-sheet liability that informed investors now price into pre-money valuations.
Investment Strategy: How to Position Around the FDA-EMA Structural Divergence
The divergence is structural, not cyclical. It will not self-correct in the near term. Several positions follow from that observation.
A portfolio long on U.S.-first regulatory strategy benefits from companies that have optimized their regulatory sequencing, clinical trial design, and IP lifecycle management for the FDA’s mechanisms — PDUFA timelines, Orange Book listing, Paragraph IV defense, and IRA-aware indication sequencing. These companies tend to generate stronger near-term FCF because U.S. launch economics remain superior.
A portfolio long on EU biosimilar manufacturing benefits from the SPC Manufacturing Waiver and the EU’s structural preference for biosimilar adoption through national tendering. EU-domiciled biosimilar manufacturers with pre-expiry stockpiling capabilities and tender-competitive cost structures are positioned to capture Day 1 share on major EU LOE events through 2030.
A portfolio short on devices heavily dependent on EU market access faces the continuing MDR compliance burden, legacy device withdrawal risk, and Notified Body capacity constraints. Unless MDR is substantively revised — a possibility under ongoing EU pharma legislation discussions, but not a near-term certainty — the EU device market will continue to see innovation drain toward the U.S.
The JCA implementation through 2025-2026 will generate the first real-world data on whether EU Joint Clinical Assessments improve or complicate national HTA outcomes. That data will be the single most important input for modeling EU commercial assumptions for drugs currently in Phase III development.
Key Takeaways
The FDA-EMA divide has moved from an operational challenge to a strategic variable. The U.S. is the dominant first-launch market for drugs and devices. The EU is losing clinical trial starts, device innovation, and first-launch position across multiple therapeutic areas simultaneously.
The IRA changes U.S. profitability for high-spend drugs in Medicare but doesn’t neutralize the U.S. pricing advantage over Europe. JCA and AMNOG window compression tighten EU commercial execution without improving speed. MDR has not improved patient safety as measured by access to innovation — it has slowed it.
The strategic insight is this: companies that treat regulatory affairs as a pure compliance function will systematically underperform companies that use FDA and EMA mechanics as commercial levers. Patent thicket construction, Orange Book listing strategy, SPC filing sequencing, JCA PICO management, and Project Orbis positioning are not regulatory tasks. They are revenue optimization decisions made years before launch.
Intelligence tools that aggregate these disparate data streams — Orange Book filings, SPC expiry dates by jurisdiction, Paragraph IV litigation dockets, EMA authorization timelines, JCA scoping documents — are now infrastructure for anyone making capital allocation decisions in pharmaceutical and medtech markets.
Data cited includes FDA CDER annual reports, EMA authorization statistics, MedTech Europe MDR survey 2024, ASCO JCO Global Oncology analysis 2025, Trinity Life Sciences JCA analysis, and Lyfegen approval-to-reimbursement timing study. Patent and SPC data sourced through DrugPatentWatch aggregation of Orange Book, USPTO, and national European patent registry filings.















")










