A deep-dive reference for pharma IP teams, portfolio managers, regulatory strategists, and institutional investors tracking generic market entry timelines.
1. What Mutual Recognition Agreements Are — and What They Are Not
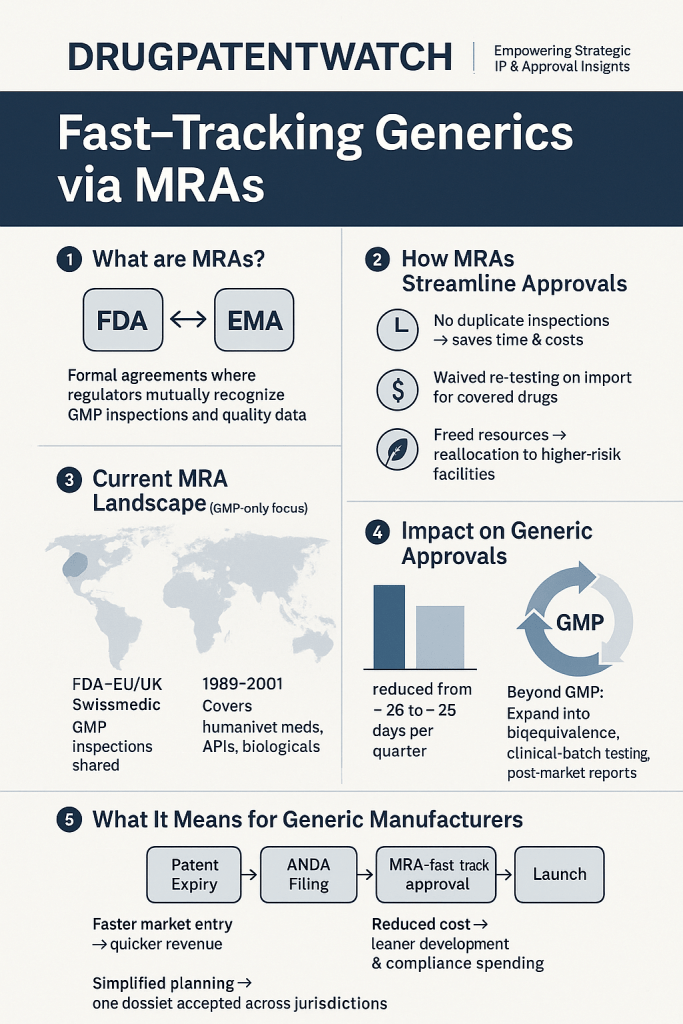
A Mutual Recognition Agreement is a formal bilateral or multilateral accord under which two or more regulatory agencies agree to accept each other’s technical assessments as sufficient for a defined regulatory decision. That definition is deceptively simple. In practice, MRAs are carefully scoped instruments that specify exactly which assessments get recognized, by which authority, under what conditions, and with what residual obligations.
For generic drugs specifically, MRAs operate across two distinct domains. The first is manufacturing inspection: one agency agrees to rely on facility assessments performed by a peer regulator rather than dispatching its own inspectors to every GMP site. The second is data recognition: one agency accepts analytical, bioequivalence, or clinical data packages that a peer regulator has already reviewed and approved, rather than re-running a full scientific evaluation from scratch.
What MRAs are not is equally important. They are not rubber stamps. An MRA that covers GMP inspections does not automatically cover data package review. An MRA covering small-molecule bioequivalence does not extend to biologics or complex injectables unless the agreement text explicitly says so. A recognition procedure that accepts a foreign approval does not typically waive post-market obligations in the destination jurisdiction. Conflating these boundaries is where regulatory teams get into trouble.
The operational consequence for generic manufacturers is that understanding an MRA’s exact scope is a precondition for building a multi-jurisdictional launch strategy. A company that files an Abbreviated New Drug Application (ANDA) with the FDA, secures approval, and then assumes that approval automatically unlocks MHRA or TGA pathways via recognition has misread the agreement architecture. Recognition procedures require specific triggering filings. They have their own timelines, their own data requirements, and their own residual review obligations.
2. The Regulatory Architecture Underneath MRAs
The ICH Framework as the Common Language
MRAs work because they rest on a shared technical foundation. The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) has, since 1990, built the common language that makes regulatory acceptance across jurisdictions conceptually possible. ICH guidelines govern everything from stability testing (Q1 series) to pharmaceutical development (Q8-Q10) to pharmacovigilance (E2 series). When two agencies both operate under ICH-compliant frameworks, the probability that their respective assessments reach compatible conclusions on chemistry, manufacturing, and controls (CMC) is high enough to justify reliance.
Without ICH alignment, MRAs collapse into political gesture. This is why every operationally significant MRA in the generic drug space, whether the FDA-EU agreement, the MHRA’s International Recognition Procedure, or the ASEAN bioequivalence MRA, sits on top of documented ICH adoption by all participating agencies. It is also why MRAs with agencies that have not formally adopted ICH guidelines remain narrow in scope or are limited to reliance rather than full mutual recognition.
The Distinction Between Reliance and Full Mutual Recognition
These two terms are frequently conflated in industry commentary. They describe fundamentally different relationships between regulatory agencies.
Reliance means an agency takes into account the work product of another agency, specifically its assessment reports, inspection findings, or approval decisions, but retains the discretion to conduct its own independent evaluation and reach a different conclusion. The WHO framework for Good Reliance Practices (GRelP), published in the Technical Report Series, formalizes this approach. The receiving agency is not bound by the reference regulator’s decision; it uses that decision as a trusted input to accelerate and inform its own assessment.
Full mutual recognition means an agency commits to accepting another agency’s determination as its own, without independent re-review, for a defined category of decisions. The FDA-EU MRA on GMP inspections operates closer to this end of the spectrum: once the operational phase was fully activated in 2019, FDA agreed to rely on EMA-member-state inspections of EU-based manufacturing sites for human medicinal products, and vice versa, removing the obligation for duplicative facility visits.
For generic manufacturers building regulatory strategy, the distinction matters enormously. A reliance pathway reduces workload and compresses timelines but does not guarantee outcome equivalence with the reference jurisdiction. A full mutual recognition pathway, when it exists for the relevant product category, can effectively make simultaneous multi-market approval feasible in a single regulatory cycle.
Key Takeaways: Regulatory Architecture
The operational value of an MRA scales directly with the scope of what is actually being recognized. Teams that map that scope precisely, including which product classes, which data types, and which residual review obligations apply, build realistic launch timelines. Teams that assume broad recognition based on headline-level agreement announcements routinely discover late that their target jurisdiction has requirements the MRA does not cover.
3. GMP Harmonization as the Load-Bearing Wall
Why Manufacturing Inspection Is the First Domino
Every generic drug approval, regardless of jurisdiction, requires demonstrated compliance with Good Manufacturing Practices at every facility involved in production. API synthesis, formulation, packaging, and testing sites all carry GMP obligations. Before any MRA on data recognition can matter, the manufacturing infrastructure has to be trusted by the receiving agency.
This is why FDA’s bilateral MRA with the EU, signed in 1998 and reaching full operational status in 2019 after a decade-long capability assessment phase, is the foundational infrastructure on which U.S.-European generic market entry strategy rests. The agreement covers human medicinal products and human biological products at facilities in EU member states and the United States. It does not currently extend to veterinary products, medical devices, or active pharmaceutical ingredients manufactured outside those jurisdictions.
The practical effect is that a generic manufacturer operating a GMP-compliant site in Germany or Ireland does not require FDA inspection before U.S. ANDA approval, provided the EMA or relevant national competent authority (the German BfArM, for example, or the Irish HPRA) has already inspected the site and found it compliant. FDA accepts that inspection as sufficient. The 35% reduction in redundant inspections documented by FDA since the agreement’s operational activation reflects this directly.
The PIC/S Network: Extending GMP Equivalence Globally
The Pharmaceutical Inspection Co-operation Scheme (PIC/S) is the mechanism through which GMP equivalence extends beyond bilateral agreements. PIC/S has 56 member authorities as of 2025, including regulators across Europe, Asia-Pacific, Latin America, and Africa. Member authorities commit to harmonized GMP standards and share inspection reports through a common database.
For generic manufacturers, PIC/S membership of the facility’s home regulator is a proxy for GMP credibility across a wide network. A site in Singapore inspected by the Health Sciences Authority (HSA), which is a PIC/S member, carries GMP standing that many destination regulators will accept without re-inspection. A site in a country whose regulator is not PIC/S-affiliated faces a much harder path to multi-market GMP recognition.
The implication for IP and regulatory strategy is that facility location decisions carry regulatory valuation consequences. A manufacturing site in a PIC/S-member jurisdiction is not just cheaper to run for compliance purposes; it is a more transferable GMP asset in licensing deals, divestitures, and co-development arrangements where the acquirer or partner needs to rely on existing regulatory standing.
IP Valuation Note: GMP Compliance Status as an Asset Class
In pharmaceutical M&A and licensing transactions, GMP compliance history at a manufacturing site is increasingly priced as a discrete asset. A facility with no FDA 483 observations in the past three inspection cycles, GMP equivalence recognition under PIC/S, and an active EU GMP certificate commands a demonstrably different licensing rate or acquisition multiple than a comparable facility with an outstanding Warning Letter. Due diligence teams that quantify this delta, rather than treating regulatory compliance as a binary pass/fail, produce more accurate asset valuations and identify more leverage in negotiations.
4. The ASEAN Bioequivalence MRA: A Full Technical Breakdown
Background and Scope
The ASEAN Mutual Recognition Arrangement on Bioequivalence Study Reports for Generic Medicinal Products was signed in November 2017 by the ten ASEAN member states: Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, the Philippines, Singapore, Thailand, and Vietnam. It covers oral solid dosage forms of generic drugs that require bioequivalence demonstration for registration.
Under the arrangement, a bioequivalence study conducted at an ASEAN-accredited bioequivalence center and accepted by one member state’s national regulatory authority (NRA) is automatically recognized by all other member states for the purpose of registration of that same generic product. The study does not need to be repeated in each country. The dossier built around the accepted study is portable across the bloc.
Accreditation Infrastructure: The Technical Prerequisite
The arrangement’s practical value depends entirely on the quality of the accredited bioequivalence centers. Each ASEAN member state is responsible for designating its own accredited centers, subject to regional peer review under the ASEAN Pharmaceutical Product Working Group (PPWG). Centers must comply with ICH E6 Good Clinical Practice guidelines, WHO bioequivalence standards, and ISO/IEC 17025 for analytical laboratory competence.
As of 2025, accredited or provisionally-accredited centers exist in Thailand, Malaysia, Singapore, the Philippines, and Indonesia. This concentration matters for strategic planning. A generic developer that needs to generate a study recognized across all ten ASEAN markets must conduct that study at a center in one of these five countries, not at a facility in the destination market. For manufacturers in Vietnam, Myanmar, or Cambodia without access to a local accredited center, the arrangement requires either contracting with an accredited center abroad or relying on foreign-generated data under the recognition mechanism.
Timeline Impact: The 6-12 Month Compression
Before the 2017 arrangement, a generic manufacturer seeking registration across all ten ASEAN markets faced the prospect of conducting separate bioequivalence studies for each jurisdiction, or at minimum submitting the same study for independent review ten times, each with its own data format requirements, reference product specifications, and review timelines. Country-level registration in ASEAN historically ranged from 12 to 36 months depending on the NRA.
The arrangement compresses bioequivalence-related review to a single accepted study. ASEAN NRAs handling a dossier supported by an already-accepted bioequivalence package have documented approval timelines averaging 6-12 months faster than pre-arrangement baselines for oral solid generics. For manufacturers with significant regional portfolios, covering 10-15 products across the bloc, the cumulative time-to-market advantage compounds into a measurable first-mover advantage in markets where therapeutic substitution rates favor the earliest approved generic.
What the ASEAN MRA Does Not Cover
The 2017 arrangement is explicitly limited to oral solid dosage forms requiring bioequivalence studies. It does not apply to injectables, topical formulations, inhalation products, or complex drug-device combinations. It does not cover BCS-based biowaivers, which require separate regulatory handling in each ASEAN NRA per their individual biowaiver policies. And it does not address CMC review, labeling requirements, or pricing and reimbursement negotiations, all of which remain fully national-level processes with no harmonization commitment.
Generic developers who treat the ASEAN MRA as a full-registration fast-track rather than a bioequivalence data fast-track build timelines that do not survive contact with the actual registration process. CMC dossier preparation for ten separate national formats, even with harmonized bioequivalence data, remains a significant workload.
IP Valuation: ASEAN Market Access as a Portfolio Asset
For companies managing generic portfolios with significant ASEAN exposure, the commercial value of MRA-recognized bioequivalence data packages is material. A study accepted under the ASEAN arrangement effectively unlocks a market exceeding 650 million people, concentrated in middle-income countries where oral solid generics capture the dominant share of pharmaceutical spending.
Investors and licensing partners are increasingly pricing ASEAN registration status at accredited centers into asset valuations. A generic product with accepted ASEAN bioequivalence data and active registrations in five or more ASEAN markets carries a materially different strategic value than a comparable product with only FDA and EMA approval, particularly for companies with distribution infrastructure in the region.
Key Takeaways: ASEAN Bioequivalence MRA
The arrangement is the most operationally complete regional bioequivalence MRA in a non-Western market. Its value is real but bounded: it compresses one step in a multi-step registration process, and that step specifically is the bioequivalence study review. Manufacturers with high-volume oral solid generics portfolios targeting Southeast Asia should be building ASEAN-accredited center relationships now, ahead of product selection, so that study placement decisions are driven by strategic site alignment rather than availability.
5. The UK International Recognition Procedure: Track-by-Track Analysis
Why the IRP Was Created
When the United Kingdom left the European Medicines Agency regulatory network on January 1, 2021, it lost access to the centralized procedure and the EU’s mutual recognition procedure, through which roughly 45% of medicines approved in the UK had previously been authorized. The MHRA initially operated a transitional reliance framework, accepting EC-authorized product information for existing products, but new approvals required a full MHRA review under domestic procedures.
The International Recognition Procedure, made available from January 24, 2024, is the MHRA’s structural response to that gap. It allows applicants holding an approval from a designated reference regulator to request MHRA recognition of that approval as the basis for a UK Marketing Authorisation, without a fully independent MHRA scientific assessment.
Designated reference regulators include: the FDA, EMA (European Medicines Agency), Health Canada, Swissmedic, the Therapeutic Goods Administration (TGA), Medsafe (New Zealand), Singapore’s HSA, the Japanese Pharmaceuticals and Medical Devices Agency (PMDA), and WHO prequalification for some categories.
Recognition Track A: The Standard Route
Recognition Track A applies to products approved by a reference regulator through a standard procedure with no outstanding safety or efficacy concerns, no Accelerated Approval equivalents, no conditions on the marketing authorization, and no major restrictions on use. For generic drugs specifically, Track A is the default route for ANDA-equivalent products approved by FDA or EMA-member-state approved products with an Article 10 generic status.
The MHRA commits to a 110-day assessment timeline under Track A, with a single clock-stop period during which the applicant can respond to MHRA questions. The assessment focuses on: verifying the reference authorization is current and unconditional, confirming qualitative and quantitative compositional equivalence between the reference-jurisdiction product and the UK product, reviewing any UK-specific labeling requirements, and confirming GMP compliance for UK-supply manufacturing sites.
For a generic manufacturer with a clean FDA ANDA approval and a UK-supply site with existing MHRA GMP standing, Track A represents a credible path to UK market authorization in approximately four months post-submission, compared to 12-18 months for a standard national procedure.
Recognition Track B: Complex Cases and Conditional Approvals
Track B applies when the reference jurisdiction approval carries conditions, was granted under an expedited or surrogate-endpoint pathway, or involves a new active substance, a hybrid application, or reliance on real-world evidence rather than conventional clinical data. The MHRA assesses these applications over 210 days with up to two clock-stops.
Track B is not a generic drug pathway in the conventional sense, because most small-molecule generics with straightforward bioequivalence demonstrations and clean reference approvals qualify for Track A. Track B becomes relevant for complex generics, locally-acting products, or products where the reference authorization was granted under the FDA’s 505(b)(2) pathway or EMA’s hybrid application Article 10(3) route, both of which involve some original data beyond standard bioequivalence.
For generic biosimilars, a category MHRA has not yet formally integrated into the IRP, neither track currently applies in a clean form. The MHRA’s biosimilar recognition pathway remains under separate development.
Labeling and Compositional Equivalence Requirements
Track A’s compositional equivalence requirement deserves more attention than most commentators give it. MHRA requires that the product supplied to the UK market be identical in qualitative and quantitative composition to the product approved by the reference regulator. This sounds straightforward but creates practical complications for manufacturers using region-specific excipients, different colorants for market differentiation, or formulation variants introduced to address regional patient preference.
A generic manufacturer who reformulated a tablet’s film coat between FDA approval and UK launch, even with no functional or bioequivalence implications, needs to resolve whether that change breaks compositional equivalence for IRP purposes. If it does, the application may fall outside Track A eligibility and require either a Track B assessment or a separate variation procedure on top of the initial recognition application. Regulatory teams building IRP timelines should map composition against the reference product at the earliest dossier preparation stage.
IP Valuation Note: MHRA IRP Status in Post-Brexit Deal Structures
In the post-Brexit M&A environment, MHRA marketing authorizations have emerged as distinct assets from EMA or EU-member-state authorizations. Acquiring an IRP-eligible product with an existing FDA or EMA reference approval significantly compresses the UK authorization timeline for the acquirer compared to building from a UK-only application. In deal structures involving generic portfolios with European and UK commercial ambitions, the presence of IRP-eligible reference approvals is material to post-close timeline projections, and therefore to purchase price.
Key Takeaways: UK International Recognition Procedure
Track A is fast (110 days), narrow in scope, and works cleanly for standard generic products with unconditional reference authorizations. The compositional equivalence requirement is a real gating factor, not a formality. Teams building UK launch timelines for generics post-FDA approval should build the IRP application in parallel with the ANDA review cycle, so that submission-ready IRP dossiers are ready to file within weeks of FDA approval.
6. FDA-EU MRA: Inspection Reciprocity and Its IP Implications
The Structure of the Agreement
The FDA-EU MRA was first signed in 1998, revised and expanded in 2017, and reached full operational status in July 2019 after a phased capability assessment process in which FDA evaluated the technical and procedural competence of each EU national regulatory authority and EMA evaluated FDA’s GMP inspection program. The assessment phase was necessary because the agreement requires documented confidence in the peer regulator’s technical capacity before inspection reliance can begin.
The agreement’s primary operational mechanism is this: for a manufacturing site located in an EU member state that has completed FDA’s capability assessment, FDA accepts the GMP inspection conducted by that member state’s national competent authority (NCA) as equivalent to an FDA inspection. Similarly, EMA-network inspectors accept FDA GMP findings for U.S.-based manufacturing sites without independent EU inspections. This reciprocity covers human medicinal products and human biologics.
What the Agreement Does Not Cover
The FDA-EU MRA explicitly excludes: API manufacturing at sites not directly involved in finished-product manufacture, veterinary medicinal products, medical devices, drug-device combination products classified as medical devices in one or both jurisdictions, and manufacturing sites in third countries supplying either market. A U.S. generic manufacturer that sources its API from a Chinese or Indian manufacturer has not resolved GMP inspection obligations for that API site through the FDA-EU MRA.
This exclusion is commercially significant. Most generic drug manufacturers sourcing APIs from India or China face full FDA and EMA inspection obligations for those sites, independent of any MRA. The supply chain inspection burden is only partially relieved by the bilateral agreement, which is an important constraint for companies with complex global supply chains.
Inspection Data Sharing: The Operational Advantage
Beyond inspection reciprocity, the FDA-EU MRA formalizes a mechanism for real-time sharing of inspection information, including warning letters, import alerts, and GMP non-compliance findings. When FDA issues a Warning Letter to an EU-based facility, that information is transmitted to the relevant EU NCA. When an EU NCA issues a GMP non-compliance decision for a U.S.-supply site, FDA receives that finding.
For generic manufacturers managing multi-jurisdictional supply chains, this data-sharing mechanism is a compliance management consideration. A facility’s GMP standing is no longer compartmentalized by jurisdiction. A finding in one regulatory ecosystem propagates to the other. Compliance teams that manage FDA and EMA inspection readiness as separate programs with different internal owners are operating an outdated model.
IP Valuation: GMP Equivalence as a Licensing Asset
In licensing and supply agreements for generic products, GMP-equivalent standing under the FDA-EU MRA is a quantifiable component of the manufacturing asset’s value. A licensor offering supply from an EU-based facility with EMA GMP certification, current under the FDA-EU MRA framework, can offer a U.S. licensing partner access to FDA-acceptable supply without requiring that partner to navigate FDA pre-approval inspections on an independent basis. That operational convenience has a price, and sophisticated licensing negotiations quantify it.
7. WHO Good Reliance Practices and the Resource-Constrained Regulator Problem
The MRA frameworks described above, whether FDA-EU, MHRA IRP, or ASEAN bioequivalence, were designed by and for agencies with substantial technical capacity. FDA employs approximately 4,000 full-time scientific staff. EMA coordinates expert review across 27 member state NCAs. The MHRA, post-Brexit, built a dedicated scientific review infrastructure.
Regulatory agencies in low- and middle-income countries (LMICs) operate under dramatically different constraints. A national regulatory authority in sub-Saharan Africa may have fewer than 50 scientific reviewers covering all product categories, from food safety to medical devices to pharmaceuticals. Conducting independent technical reviews of complex generic dossiers, including CMC assessment, bioequivalence data review, and risk-benefit analysis, at scale is not operationally feasible for most LMIC NRAs.
This is not a failure of will. It is a resource and capacity reality that conventional MRA frameworks, which require technical reciprocity, were not designed to address.
WHO GRelP as the Practical Framework
The WHO framework for Good Reliance Practices formalizes what most LMIC NRAs were already doing informally: using approval decisions from stringent reference regulators, primarily FDA, EMA, and Health Canada, as the basis for their own regulatory decisions without independent full technical review. GRelP provides a structured methodology for doing this responsibly.
Under GRelP, the receiving NRA performs a defined subset of assessments: reviewing the reference regulator’s summary basis of approval for red flags specific to the local patient population (pharmacogenomic differences, endemic disease interactions, local excipient availability), verifying that the manufacturing sites supplying the local market have current GMP standing, and confirming that labeling is appropriate for local context. The full CMC and clinical assessment is delegated to the reference regulator’s already-completed work.
WHO prequalification operates as a parallel and complementary mechanism. WHO prequalification is not an NRA, but its technical reviews are rigorous enough that most LMIC NRAs treat a WHO prequalification as equivalent to a stringent-regulator approval for reliance purposes. For generic HIV antiretrovirals, antimalarials, and tuberculosis treatments, WHO prequalification has been the operational fast-track that put affordable generics into procurement programs at the national level across Africa and South Asia.
African Medicines Agency: The Emerging Centralization Option
The African Medicines Agency (AMA), whose establishing treaty entered into force in November 2021 and which is now operational in a limited capacity under African Union governance, represents the structural evolution of reliance frameworks in Africa. Rather than each African NRA managing its own reliance procedures independently, the AMA concept is that a centralized AMA scientific committee would conduct a single consolidated review, relied upon by all member states.
The AMA is not yet operational at scale for generic drug assessments. Governance, funding, and technical infrastructure are still being built. But its existence creates an investment thesis for generic manufacturers with broad African commercial ambitions: building a relationship with the AMA review process now, during its operational build-out, positions companies to benefit first from centralized fast-track pathways once they become active.
Key Takeaways: WHO GRelP and LMIC Markets
WHO prequalification remains the most reliable operational fast-track for generic access to LMIC procurement markets. For companies manufacturing off-patent HIV, malaria, and TB generics, WHO prequalification is the de facto MRA for markets across sub-Saharan Africa, South Asia, and parts of Southeast Asia. The AMA represents a longer-term structural opportunity that is real but not yet bankable for five-year commercial planning.
8. Paragraph IV Strategy in an MRA World
How MRA Timelines Interact with Hatch-Waxman Mechanics
U.S. generic strategy for patent-protected reference listed drugs (RLDs) runs on Hatch-Waxman mechanics. An ANDA filer challenging an Orange Book-listed patent files a Paragraph IV certification, certifying that the listed patent is invalid or will not be infringed by the generic product. The RLD patent holder has 45 days from notice of the Paragraph IV certification to sue for infringement, triggering a 30-month stay on FDA ANDA approval. The first ANDA filer to file a Paragraph IV certification earns 180 days of generic exclusivity, during which FDA cannot approve a second generic.
MRA frameworks layer on top of this U.S.-specific mechanics in ways that strategic teams have not fully modeled. The critical interaction is this: in jurisdictions covered by MRA or IRP-style recognition procedures, the U.S. ANDA approval is the triggering event that enables fast-track recognition applications. The 180-day exclusivity period a first filer earns in the U.S. does not extend to UK, EU, or ASEAN markets. A second-to-file ANDA applicant that loses 180-day exclusivity in the U.S. can potentially launch in the UK, Australia, or ASEAN markets simultaneously with or ahead of the U.S. first filer, if it submits IRP or TGA reliance applications at the time of ANDA approval rather than after U.S. launch.
This represents a genuine strategic asymmetry that most Paragraph IV strategy discussions do not adequately address. The race for U.S. 180-day exclusivity is one competition. The race for ex-U.S. first launch via MRA pathways is a separate competition, and the leaders in each do not automatically coincide.
Patent Linkage and MRA Jurisdictions
FDA’s Orange Book system links ANDA approval to patent expiry and litigation status through a formal statutory mechanism. The MHRA, EMA, Health Canada, and TGA do not operate equivalent patent linkage systems, at least not with the same statutory force. In the IRP context, MHRA does not search for Orange Book-listed patents or consider U.S. patent litigation status when processing an IRP application. An IRP application for a generic product that is under a 30-month stay in the U.S. can, in principle, receive MHRA recognition and UK marketing authorization while the U.S. approval remains frozen.
Whether this creates a commercial launch opportunity in the UK depends on the IP landscape there, specifically on whether equivalent UK patents are in force and whether the RLD holder has enforcement options. But the regulatory pathway in the UK is independent of U.S. patent linkage, and teams that assume the 30-month stay pauses all global progress on a Paragraph IV product are leaving ex-U.S. launch opportunities on the table.
Key Takeaways: Paragraph IV and MRA
Paragraph IV filers should build multi-jurisdictional MRA pathway analysis into pre-filing strategy, not post-approval commercial planning. The interaction between U.S. patent linkage mechanisms and MRA recognition timing in ex-U.S. jurisdictions creates launch sequence opportunities that are invisible to teams whose strategic modeling is U.S.-centric.
9. IP Valuation Considerations When MRA Access Is a Core Asset
Quantifying the Regulatory Asset Premium
Pharmaceutical IP valuation typically anchors on patent life remaining, exclusivity periods, and revenue projections discounted for probability of technical and regulatory success. MRA access is not yet consistently priced as a discrete asset in most pharma valuation models, but its economic consequence is material and increasingly quantifiable.
Consider a generic product with FDA ANDA approval, an IRP-eligible reference authorization, current ASEAN bioequivalence data at an accredited center, and a PIC/S-member manufacturing site. Compared to an otherwise identical generic with FDA approval only, this product has:
A materially shorter time-to-revenue in the UK, Australia, Canada, Singapore, and select ASEAN markets, by 12-18 months on average. An inspection-cost reduction over its commercial life, given GMP reciprocity under active MRA frameworks. A broader licensing value to partners seeking multi-jurisdictional commercial rights, because the regulatory infrastructure to enter those markets is partially built.
In formal NPV models, a 12-month compression of market entry timing in a market generating $20M-$50M annually translates directly to additional discounted cash flow of $15M-$40M at typical pharma discount rates. That delta belongs in asset valuations and licensing negotiations, not treated as a bonus discovered post-deal.
MRA-Eligible Dossiers as Licensing Leverage
In out-licensing negotiations, the party with an MRA-eligible dossier holds structural leverage. They are not just licensing a product; they are licensing a regulatory package that reduces the licensee’s time and cost to generate revenue in multiple jurisdictions. That is a bundled value proposition. Sophisticated licensors price the MRA-eligible status of their dossiers explicitly, whether as a higher upfront fee, a higher royalty rate, or a shorter exclusivity grant, because they can demonstrate the incremental commercial value it delivers to the licensee.
Licensees, correspondingly, should conduct regulatory due diligence on MRA eligibility as a discrete step in licensing due diligence. Questions to resolve before signing: Does the reference authorization qualify under the relevant IRP or recognition procedure? Is the manufacturing site GMP-equivalent in the target jurisdiction? Are bioequivalence data current and generated at an accredited center recognized in the target market? Are there any compositional differences between the reference-jurisdiction product and the intended commercial product that could disqualify IRP Track A eligibility?
Evergreening and MRA Interactions
Branded pharmaceutical companies use evergreening strategies, specifically patent term extensions, formulation patents, new indication filings, and pediatric exclusivity, to extend market exclusivity beyond the original compound patent expiry. MRAs do not inherently accelerate the erosion of evergreening protections, but they do change the competitive response timeline once the IP position erodes.
When a compound patent expires in the U.S. and the relevant Orange Book patents are successfully challenged or expire, MRA pathways allow generic manufacturers to convert that U.S. approval into multi-market approvals with a speed that compresses the branded company’s ability to shift market share to a next-generation protected product before generics enter multiple jurisdictions simultaneously. A branded company whose evergreening strategy depends on sequential country-by-country generic entry, with several years of relative protection in each ex-U.S. market after U.S. generic entry, faces a more compressed timeline in an MRA-enabled world.
10. Post-Market Surveillance: The Gap That Can Unwind a Fast-Track
The Core Accountability Problem
MRA and reliance procedures accelerate market entry by compressing the pre-approval review cycle. They do not, by design, create a post-market surveillance network to match. The receiving agency relied on the reference regulator’s pre-approval assessment. It may not have built parallel pharmacovigilance infrastructure to independently monitor the product once it enters its market.
This creates a structural accountability gap. When an adverse event signal emerges post-launch, the receiving agency may lack the pharmacovigilance data on its own population to independently confirm or refute the signal. If the adverse event is driven by a population-specific factor, a pharmacogenomic difference, a co-morbidity pattern more prevalent locally, or a drug interaction pattern shaped by different co-medication practices, the reference regulator’s pharmacovigilance system may not detect it because the reference population does not exhibit the same risk.
The FDA’s Accelerated Approval program has been criticized repeatedly for weak post-market enforcement of confirmatory study commitments. In the MRA context, this problem is compounded: not only may confirmatory studies be delayed, but the receiving agency may have no independent safety database from its own market to trigger regulatory action independent of the reference regulator’s findings.
MHRA IRP’s Partial Response: Track B Monitoring
Recognition Track B, which applies to conditionally-approved products and those relying on surrogate endpoints or real-world data, requires applicants to submit ongoing monitoring reports to the MHRA, including periodic safety update reports (PSURs) on a defined schedule and notification of any safety-related variations in the reference jurisdiction. This creates a formal conduit: if the FDA or EMA imposes a new risk mitigation requirement on a Track B product, the MHRA learns of it through the required notifications and can act in the UK market accordingly.
Track A does not carry equivalent structured monitoring requirements. MHRA relies on the standard PSUR system and the EU-UK MRA information-sharing channels, where they function, for safety signal awareness. For standard generics with well-characterized safety profiles, this is defensible. For complex generics, modified-release formulations, or products with narrow therapeutic indices, it is a thinner post-market safety net than the pre-approval assessment phase would suggest.
WHO’s Collaborative Pharmacovigilance Initiative
WHO operates collaborative pharmacovigilance centers through the Uppsala Monitoring Centre (UMC), which aggregates individual case safety reports from member country pharmacovigilance systems into a global signal detection database (VigiBase). LMICs relying on WHO prequalification or GRelP for initial approvals are encouraged to feed post-market safety data into VigiBase so that global signal detection can compensate for individual-country pharmacovigilance gaps.
The system works imperfectly. Underreporting rates in most LMIC pharmacovigilance systems are high, as high as 94% by some estimates, meaning most adverse events that occur are never entered into VigiBase. For generic products entering LMIC markets via reliance on WHO prequalification, the post-market safety network is effectively the branded reference product’s global pharmacovigilance database plus whatever the local NRA can generate from its own reporting infrastructure.
11. Biosimilars and MRAs: The Frontier That Has Not Opened Yet
Why Biosimilar Recognition Is Structurally Harder
MRAs for small-molecule generics rest on bioequivalence as the primary scientific standard. Two formulations of the same molecule, manufactured by different processes, are therapeutically equivalent if they deliver the same active ingredient to systemic circulation at the same rate and extent under the same conditions. That is a testable, reproducible, and highly harmonized scientific standard across all major regulatory agencies. Once you have bioequivalence, you have the analytical foundation for data recognition.
Biologics do not work this way. A biosimilar is not chemically identical to its reference biologic, because protein-based therapeutics are defined by their manufacturing process. The three-dimensional structure, glycosylation pattern, aggregate content, and immunogenic potential of a biologic depend on the cell line, fermentation conditions, purification steps, and formulation of the specific manufacturer’s process. Two manufacturers using different processes to produce a nominally identical monoclonal antibody will produce molecules that are analytically similar but not identical.
This means biosimilar comparability exercises are manufacturing-process-specific rather than molecule-specific. A biosimilar regulatory package approved by FDA for trastuzumab produced by Manufacturer A cannot be simply recognized by MHRA for trastuzumab produced by Manufacturer A’s EU facility without a separate manufacturing comparability exercise confirming that the EU-facility process produces a product analytically comparable to the U.S.-facility reference package. The analytical complexity of that exercise is orders of magnitude greater than confirming bioequivalence for a small-molecule generic.
Current State of Biosimilar MRA Development
No comprehensive biosimilar MRA exists as of 2025. What does exist is a set of bilateral information-sharing arrangements and joint review pilots for biosimilars between FDA and EMA, operating under the FDA-EMA Collaboration on Biosimilar Development initiative. These arrangements allow FDA and EMA scientific reviewers to share assessment reports, participate in joint expert discussions, and align on methodological approaches to biosimilar comparability, but they do not create automatic data recognition or approval reliance for biosimilar applications.
The MHRA’s IRP does not currently include biosimilar products as an eligible category for recognition. The ASEAN MRA covers only oral solid generics. WHO prequalification has begun to address biosimilars in the context of insulins and selected monoclonal antibodies, but recognition by national NRAs of WHO prequalified biosimilars is not yet systematically operationalized.
The Biosimilar Interchangeability Question
In the U.S., FDA can designate an approved biosimilar as ‘interchangeable’ with its reference biologic if the biosimilar sponsor demonstrates, through switching studies, that alternating between the biosimilar and the reference product does not produce greater risk than using the reference product alone. Interchangeability designation allows pharmacists in states permitting automatic substitution to dispense the biosimilar without prescriber intervention, equivalent to generic substitution for small molecules.
No equivalent of biosimilar interchangeability designation exists in the EU, UK, Australia, or most Asian markets. EMA position on interchangeability is that it is a national-level decision, not a designation EMA grants. This creates a structural asymmetry: an FDA interchangeability designation for a biosimilar cannot be leveraged through any recognition procedure in EU or UK markets, because the regulatory category does not translate. The interchangeability designation is jurisdictionally trapped in the U.S.
Key Takeaways: Biosimilars and MRAs
Biosimilar developers cannot currently use MRA or reliance pathways to convert a single regulatory approval into fast-tracked multi-market authorizations in the way small-molecule generic developers can. Each major market requires a substantially complete biosimilar comparability dossier. The investment in multi-market biosimilar regulatory strategy is higher per product, per jurisdiction, than the equivalent investment for small-molecule generics. Teams projecting ex-U.S. biosimilar launch timelines based on generic drug MRA assumptions are building unreliable revenue forecasts.
12. Geopolitical Risks and Agreement Fragility
When Politics Overrides Regulatory Logic
MRAs are regulatory instruments, but they are also political agreements. They require active governmental will to maintain, and they can be suspended, renegotiated, or effectively nullified by political decisions that have nothing to do with technical regulatory competence.
The clearest recent example is the 2021 dispute between the EU and the United Kingdom over COVID-19 vaccine supply, during which the EU threatened to restrict vaccine exports under Article 122 of the Treaty on the Functioning of the European Union. While this dispute did not formally suspend the post-Brexit pharmaceutical regulatory arrangements, it demonstrated that the political environment could destabilize supply and regulatory cooperation mechanisms in ways that no legal text fully anticipates.
More structurally, the U.S.-EU relationship has undergone significant strain over trade, technology competition, and foreign policy. The FDA-EU MRA depends on mutual confidence and operational cooperation that could be compromised if broader trade tensions lead to formal or informal restrictions on regulatory information sharing. The agreement has no force majeure provision for geopolitical disruption.
Concentration Risk in Reference Regulator Networks
IRP and GRelP reliance frameworks concentrate regulatory dependence on a small number of reference regulators, primarily FDA, EMA, and Health Canada. If any of these agencies undergoes significant capacity reduction, through budget cuts, political pressure, or personnel attrition, the entire downstream reliance network is degraded. Countries relying on FDA’s technical assessments for their own registration decisions have no fallback if FDA’s review quality or throughput declines.
This concentration risk is not theoretical. FDA’s generic drug review program has faced significant pressure from user fee funding cycles, and any disruption to PDUFA or GDUFA reauthorizations can compress review timelines, which propagates to jurisdictions that treat FDA approval as the triggering event for their own recognition procedures.
Key Takeaways: Geopolitical and Structural Risk
Build MRA dependency into supply chain risk modeling. A product portfolio that relies on FDA-EU MRA GMP equivalence for EU supply of a U.S.-authorized product is exposed to bilateral agreement disruption in ways that a portfolio with independent GMP certifications in both jurisdictions is not. The insurance cost of maintaining independent regulatory standing in key markets is a legitimate portfolio risk management expense.
13. What a Future Global MRA Architecture Could Look Like
Joint Clinical Trial Reviews
The most significant expansion of MRA scope under discussion is joint clinical trial review, under which two or more agencies simultaneously assess the same pivotal study data and reach a coordinated approval decision. FDA and EMA have conducted joint scientific advice sessions for complex generics and some new molecular entities under the FDA-EMA Parallel Scientific Advice (PSA) program since 2004. This is advisory, not regulatory, but it establishes the collaborative infrastructure that could support joint review.
For complex generics requiring clinical endpoint studies, specifically complex injectables, liposomal formulations, ophthalmic drug products, and certain inhalation products where bioequivalence cannot be demonstrated by conventional pharmacokinetic methods, joint clinical review could compress multi-market approval timelines from sequential years-long processes into near-simultaneous decisions. The procedural and legal barriers are significant: agencies in different jurisdictions operate under different statutory authorities and cannot legally co-sign each other’s approval documents. But technical alignment before individual national approvals can be functionally equivalent in reducing review time and eliminating duplicative data requirements.
Harmonized Real-World Evidence Standards
Real-world evidence (RWE) from electronic health records, claims databases, and patient registries is increasingly used to support label expansions, biosimilar indication extrapolation, and post-market safety monitoring. No harmonized global standard for RWE quality in regulatory submissions currently exists. FDA’s RWE framework guidance (2023) and EMA’s RWE methodological framework are compatible in many respects but diverge on key methodological requirements for confounding adjustment, data quality standards, and study design transparency.
A future MRA or harmonization agreement that establishes mutually recognized RWE standards would create the regulatory infrastructure for post-approval data generated in one jurisdiction to support label changes in another. For generic manufacturers seeking to expand indications or update labeling based on post-market data, this would represent a material expansion of MRA value beyond initial approval.
Digital GMP Inspection and Remote Assessment
COVID-19-era experience with remote and hybrid GMP inspections has generated a body of evidence on the feasibility of conducting facility assessments without physical inspector presence. FDA, EMA, and several other agencies conducted successful remote inspections using video inspection technology, real-time document sharing, and pre-submitted process validation data during 2020-2022.
A formalized remote inspection protocol, standardized across MRA-partner agencies, would reduce the geographic and logistical constraints on expanding GMP equivalence to manufacturing sites in countries currently outside PIC/S or existing MRA networks. This would extend the GMP recognition framework to additional manufacturing jurisdictions, increasing supply chain flexibility for generic manufacturers sourcing from a wider range of countries.
14. Investment Strategy for Portfolio Managers
The MRA Premium in Generic Portfolio Valuation
For institutional investors evaluating generic pharmaceutical companies, MRA capabilities translate into quantifiable commercial advantages that should be priced into equity and debt analysis. The key metrics to assess are:
Percentage of the company’s product portfolio in MRA-eligible categories across target markets. Number of active registrations in MRA/reliance jurisdictions beyond the U.S., reflecting realized versus potential MRA value. Manufacturing footprint coverage relative to PIC/S membership and active FDA-EU MRA standing. Pipeline of ANDA or dossier applications in products where IRP or ASEAN recognition would materially accelerate ex-U.S. revenue generation.
Companies with high MRA utilization rates, meaning they are consistently filing IRP applications within three to six months of FDA ANDA approval and building ASEAN bioequivalence at accredited centers during rather than after U.S. development, generate ex-U.S. revenue faster than competitors running sequential regulatory programs. Over a portfolio of 20-30 products, that systematic advantage compounds into a durable speed-to-market differential.
Screening Criteria for Generic Drug Investments
Portfolio managers evaluating generic pharmaceutical companies for investment should apply the following screening criteria related to MRA capabilities:
Does the company maintain active GMP certifications at manufacturing sites covered by the FDA-EU MRA or PIC/S equivalence, or does it rely exclusively on site-specific FDA inspections? Does the company have a systematic process for filing IRP applications in the UK, TGA-reliance applications in Australia, and Health Canada reliance applications for Canadian market access immediately following FDA ANDA approval, or does it treat ex-U.S. markets as sequential opportunities? For companies with ASEAN commercial exposure, does the company conduct bioequivalence studies at ASEAN-accredited centers as a standard practice for oral solid generics, or does it generate ASEAN-specific studies after U.S. development?
A company that answers no to these questions consistently is leaving systematic ex-U.S. revenue on the table through regulatory execution delays. A company that answers yes consistently has built a regulatory operating model that maximizes MRA value across its entire portfolio, and that model is a durable competitive advantage.
M&A Diligence: MRA-Specific Checklist
In pharmaceutical M&A diligence, MRA-related items to investigate include: current GMP inspection status and currency of certificates at all manufacturing sites, including the date of last inspection in each jurisdiction and whether any outstanding observations exist; full inventory of IRP, TGA reliance, and Health Canada reliance applications filed or pending for the target portfolio; ASEAN registration status and bioequivalence study center affiliations for products with Southeast Asian commercial exposure; and any IP or contractual constraints that would prevent the acquirer from using the target’s reference authorizations as the basis for recognition applications in new jurisdictions.
An acquirer that completes a generic portfolio acquisition and then discovers that the target’s manufacturing sites are due for MHRA or TGA re-inspection within 18 months, with outstanding observations from prior inspections, has inherited a regulatory risk that compresses the ex-U.S. commercial timeline materially. Pricing that risk correctly requires MRA-specific diligence that goes beyond standard FDA compliance review.
15. Key Takeaways by Segment
For Regulatory Affairs Teams
MRA pathways are not automatic. They are procedural mechanisms that require specific triggering filings, meet compositional equivalence requirements, and satisfy manufacturing GMP standing in the destination jurisdiction. The time to build an IRP or reliance application is during U.S. ANDA development, not after FDA approval. Parallel dossier preparation for key ex-U.S. recognition markets should be standard operating procedure for any generic product with significant commercial potential beyond the U.S.
Biosimilar MRA pathways do not currently exist in a meaningful form. Teams projecting biosimilar launch timelines in UK, Australian, or ASEAN markets should build those timelines on independent full-dossier submission assumptions, not on reliance or recognition assumptions.
For IP and Business Development Teams
MRA-eligible regulatory packages are licensable assets with quantifiable value. The ability to deliver an IRP-eligible dossier or an ASEAN-recognized bioequivalence package to a licensing partner is a component of deal economics that should be priced explicitly, not absorbed as background noise in royalty rate negotiations.
Patent strategy in Paragraph IV filings should account for ex-U.S. recognition pathway timing. The window between U.S. ANDA approval and IRP or TGA recognition is a commercially sensitive period where first-mover advantage in ex-U.S. markets can be established independent of U.S. exclusivity status.
For Portfolio Managers and Institutional Investors
Companies with systematic MRA execution capabilities, meaning they are capturing IRP, TGA, and Health Canada recognition pathways as a standard post-FDA approval process, are generating faster ex-U.S. revenue than competitors running sequential programs. This is a screening criterion for investment selection and a diligence item in M&A. The economic value of multi-market simultaneous launch capability, compared to sequential market entry, is material at the portfolio level and should be modeled explicitly in revenue projections.
For R&D and Manufacturing Leadership
Manufacturing site decisions have long regulatory tails. A decision to source API from a non-PIC/S-member country, or to locate a formulation site outside the FDA-EU MRA framework, imposes inspection costs and timeline risks that compound across every product manufactured at that site over its commercial life. GMP compliance architecture should be designed with MRA eligibility as an explicit design criterion, not as a retrospective compliance exercise.
The future of MRA expansion, toward joint clinical reviews, harmonized real-world evidence standards, and digital inspection protocols, will progressively reward manufacturers and regulatory teams that have built ICH-aligned processes and multi-agency relationships now. The organizations that will benefit most from the next generation of MRA frameworks are the ones treating regulatory harmonization as a strategic investment today.


 Tell You")





(2) Goldmine: How Pharma Extracts Maximum IP Value from Modified Drugs")

















