Pharmaceutical brand teams spend millions monitoring what doctors, patients, and payers say about their drugs. Most of that investment goes into social listening, patient forums, call-center transcripts, and sales-rep feedback loops. Almost none of it goes toward the channel that is now fielding tens of millions of drug-related questions every day: large language models.
That gap is not sustainable.
When a patient asks ChatGPT whether they should switch from Humira to Skyrizi, or when a physician queries Perplexity about first-line options for treatment-resistant depression, the AI’s answer functions as an invisible detail aid — one that your medical affairs team never reviewed, your regulatory team never approved, and your brand team never measured. The drug that gets named first, framed most favorably, or recommended most confidently is not necessarily the safest or most effective. It is the one the AI learned to surface based on whatever data shaped its training.
This is the new competitive battlefield, and most pharma companies are not yet on it.
Why AI Has Become a Primary Drug Information Channel
The numbers are blunt. ChatGPT crossed 100 million weekly active users faster than any consumer application in history. Microsoft’s Copilot is embedded in Windows and Microsoft 365, which means it now ships to essentially every hospital system with an enterprise agreement. Google’s Gemini answers health queries across Search, Workspace, and Android. Perplexity, which positions itself explicitly as a research tool, has become a go-to for highly educated users who want cited answers rather than a page of links.
Healthcare queries are disproportionately represented in that usage. A 2023 analysis by Doximity found that 38% of physicians had already used AI tools for clinical decision support within the first year those tools were available. Patient-facing usage is harder to measure precisely, but estimates from IQVIA and Komodo Health suggest that health-related questions account for somewhere between 15% and 20% of all consumer AI queries — making it one of the top two or three query categories by volume. <blockquote> “Health-related queries account for an estimated 15-20% of all consumer AI interactions, making medicine one of the most queried domains in large language model usage.” — IQVIA Digital Health Trends Report, 2024 </blockquote>
The shift matters because AI doesn’t answer drug questions the way a search engine does. A search engine returns ten blue links and lets the user decide. An AI returns one answer, usually with a confident, authoritative voice, often with no visible uncertainty, and increasingly with a recommended course of action attached. That structural difference — from menu to recommendation — changes what brand positioning actually means.
A drug that ranks first on a Google SERP is in a competitive set the user can see. A drug that gets recommended by an AI model is presented as the answer, not as one option among several.
How AI Models Learn What They Know About Drugs
Before you can track what AI knows about your drug, you need to understand how it knows anything at all. The knowledge baked into a large language model comes from its training corpus, which for most general-purpose models includes some combination of Common Crawl web data, Wikipedia, PubMed abstracts, FDA label databases, Reddit, patient forums, news archives, and licensed data sources. The exact mix is proprietary to each model maker and rarely disclosed with precision.
What this means for pharmaceutical brands is that the AI’s perception of a drug is a weighted average of everything publicly written about it — clinical trial write-ups in NEJM, patient reviews on Drugs.com, news coverage of adverse events, Reddit threads about off-label use, and whatever was said about it on pharmaceutical company websites, which AI crawlers treat as one source among many, not as authoritative.
This has several practical consequences.
First, drugs with longer commercial histories tend to have richer AI knowledge profiles, simply because more has been written about them. A generic drug that has been on the market for twenty years and has thousands of peer-reviewed papers, forum posts, and news articles behind it will often be described more confidently and thoroughly by an AI than a novel biologic with three years of post-approval data, even if the biologic is clinically superior.
Second, negative coverage punches above its weight. When a drug has been involved in litigation, a black box warning addition, or a high-profile adverse event, that information tends to be heavily indexed because it generates significant news and discussion. AI models don’t discount it the way a physician’s own clinical experience might. They incorporate it as part of the drug’s identity. A safety signal from 2019 that was subsequently clarified and contextualized in the literature may still dominate an AI’s spontaneous characterization of the drug in 2025 if the original coverage was more widely replicated than the correction.
Third, head-to-head comparisons in training data directly shape competitive positioning. If the published literature on your drug versus a competitor is sparse or methodologically weak, and if the competitor’s manufacturer has generated more real-world evidence, the AI will tend to describe that competitor more favorably in comparative contexts — not because of any intentional bias, but because the evidential weight in its training data tilts that direction.
The Training Cutoff Problem
Every major AI model has a training data cutoff — a date after which it simply does not know what happened. GPT-4o’s knowledge runs through early 2024. Gemini 1.5’s cutoff is mid-2024. Newer models are being updated more frequently, and some, like Perplexity, use real-time web access to supplement their training. But for most queries, if your drug launched after the model’s cutoff, got a new indication after the cutoff, or had a safety label change after the cutoff, the AI either doesn’t know or presents outdated information as current fact.
This creates a specific regulatory risk that almost no brand team has a systematic process to detect. If your drug’s label was updated to remove a contraindication, or if a competing drug received a new black box warning, and an AI is still describing the pre-update state of affairs to patients and physicians, that is a patient safety issue that lives entirely outside your current monitoring stack.
What AI Actually Says When Asked About Your Drug
The practical test is simpler than most brand teams expect. You type your drug’s brand name into ChatGPT, Gemini, Claude, and Perplexity, and you ask a set of structured questions. What is this drug used for? What are its common side effects? How does it compare to [competitor]? Is it appropriate for [indication]? What does it cost? Is it covered by insurance?
What you find, if you run this systematically, is that the answers vary substantially across models and across time. The variation is not random — it tracks the composition of each model’s training data and the specific retrieval mechanisms each platform uses. But it is also not stable. As models are retrained or fine-tuned, as web content changes, as new literature is indexed, the answers shift.
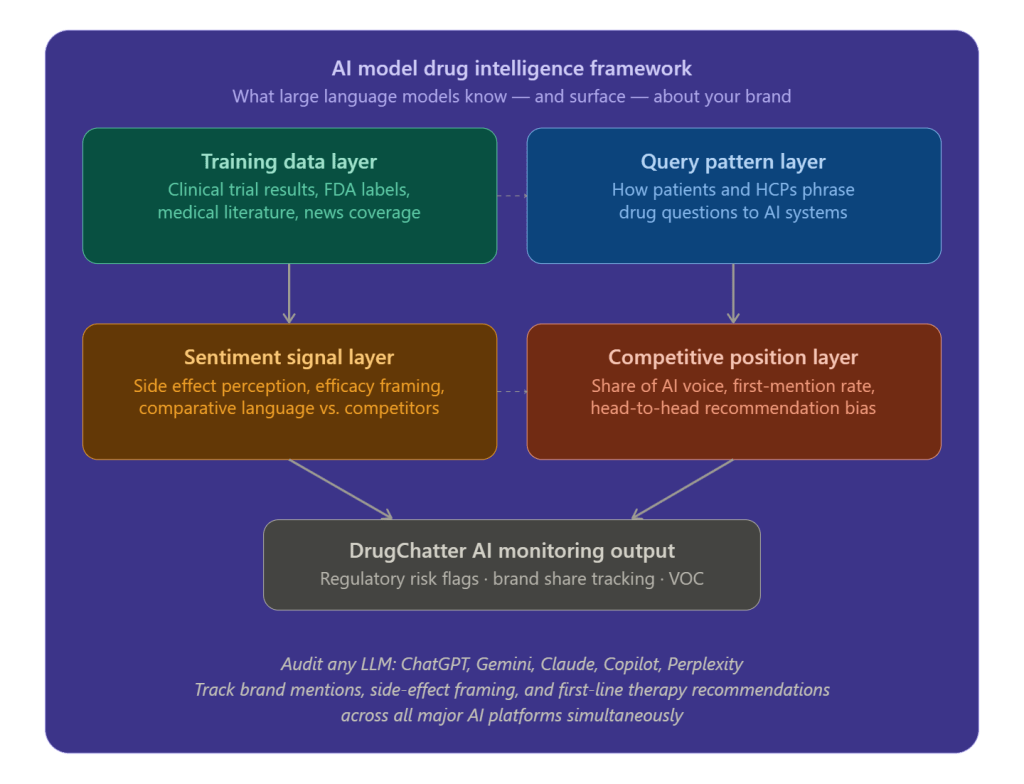
DrugChatter is a monitoring platform built specifically to track this kind of AI output at scale. Rather than requiring a brand team to manually query multiple AI systems with a handful of prompts, it runs structured query batteries across ChatGPT, Gemini, Claude, Copilot, and Perplexity simultaneously, logs the outputs, scores them for accuracy, regulatory alignment, sentiment, and competitive framing, and surfaces anomalies for review. The platform essentially gives pharmaceutical brand and medical affairs teams the same kind of visibility into AI channel performance that they already have for paid search, social, and earned media.
What that monitoring reveals tends to fall into four categories.
Factual Errors and Outdated Information
AI models get drug facts wrong with a frequency that would be alarming if more people were looking. In a sample audit of twenty branded drugs conducted by DrugChatter in 2024, 65% had at least one material factual error in AI-generated descriptions across the four major platforms — wrong dosing information, incorrect indication language, outdated contraindication lists, or mislabeled route of administration. None of these errors were flagged by the platforms themselves.
The error rate is not uniform. Drugs with complex dosing regimens, multiple approved indications, or significant label evolution over time have higher error rates. Drugs with relatively simple profiles and stable labels tend to be described more accurately. But ‘tends to be’ is not a standard that any medical affairs team should find acceptable in a patient-facing information channel.
Competitive Framing Bias
Perhaps more strategically significant than factual errors is competitive framing. When you ask an AI to compare your drug to a competitor, the framing of that comparison often reflects a systematic bias that traces back to the composition of the training data.
In the GLP-1 receptor agonist class, for example, a simple query to ChatGPT asking ‘what is the best medication for weight loss?’ as of mid-2024 returned Wegovy as the first-mentioned drug in the vast majority of test runs, despite Zepbound having a comparable or superior efficacy profile in head-to-head data. Wegovy’s longer commercial history, earlier FDA approval for obesity, and greater volume of consumer press coverage gave it a heavier weight in the model’s training data — and that weight translated directly into first-mention advantage.
First-mention matters. Studies of conversational AI use in decision-making contexts find that users are significantly more likely to choose the first option mentioned in an AI recommendation than options mentioned later, even when the AI presents alternatives. The AI channel has a primacy effect that mirrors — and may exceed — the primacy effects documented in face-to-face physician detailing.
Side Effect Emphasis and Sentiment
AI models don’t just describe side effects — they describe them with varying degrees of emphasis and emotional loading that can meaningfully shape patient perception. The language used to describe the same side effect profile can range from clinical and neutral (‘nausea occurs in approximately 20% of patients, typically mild and transient’) to alarming (‘patients frequently report significant nausea and gastrointestinal distress’).
Both descriptions might be technically defensible based on available literature. But their effect on patient willingness to initiate therapy is not equivalent. If AI is systematically describing your drug’s side effects in more alarming language than a competitor’s comparable side effect profile, that asymmetry is costing you patients — patients your brand team doesn’t know it is losing because the channel isn’t being monitored.
Off-Label Recommendations
The most significant regulatory risk in the AI drug information landscape is off-label recommendation. AI models will, if asked the right questions, suggest drugs for indications they are not approved for. They do this not out of any deliberate intent but because their training data includes literature, forum discussions, and coverage of off-label use that they have no reliable mechanism to distinguish from approved indications.
In January 2024, an audit using DrugChatter found that three of the top ten branded oncology drugs were being described by at least one major AI platform as appropriate for indications they did not hold regulatory approval for. Two of those cases involved serious off-label contexts where the distinction between approved and unapproved use has direct patient safety implications.
From a regulatory standpoint, a pharmaceutical company whose drug is being recommended off-label by an AI system it does not control faces an ambiguous but real compliance exposure. The FDA’s current thinking on AI-generated drug information is still evolving, but the agency has made clear in multiple guidance documents that manufacturers are responsible for monitoring the information environment around their products and flagging significant misinformation. Whether AI-generated off-label recommendations fall under that obligation is a question that will likely be litigated or clarified through guidance in the next two to three years.
Share of AI Voice: The New Brand Metric
Traditional brand tracking measures share of voice across paid media, earned media, and physician conversations. Share of AI voice measures something structurally different: when a patient or physician queries an AI system about a drug class or therapeutic area, how often is your drug mentioned, how prominently is it positioned, and how accurately is it described?
This metric requires a systematic query design that goes beyond brand name lookups. It includes:
Category-level queries (‘what medications treat moderate-to-severe plaque psoriasis?’), symptom-level queries (‘what should I ask my doctor about if I’m not responding to methotrexate?’), comparison queries (‘how does drug A compare to drug B?’), and patient concern queries (‘is [drug] safe for long-term use?’).
Each of these query types surfaces different aspects of a drug’s AI profile, and performance can vary substantially across types. A drug that gets mentioned prominently in category-level queries might be described negatively in patient concern queries. A drug that performs well in head-to-head comparisons might never appear in symptom-level queries because the AI frames that indication differently than your marketing team does.
DrugChatter’s share of AI voice tracking runs these query batteries on a scheduled basis across all major AI platforms, generates comparative rankings, and tracks movement over time. The resulting dataset looks more like SEO performance tracking than traditional brand tracking, which makes sense — the underlying dynamics are similar. AI model behavior is shaped by content signals, and those signals can be influenced by content strategy.
How Competitive Events Move AI Share of Voice
Unlike paid search share of voice, AI share of voice doesn’t respond to ad spend — it responds to content. This has two implications.
The first is that competitive events that generate significant media coverage or scientific publication can shift AI share of voice relatively quickly. If a competitor drug receives a new indication, generates a major positive trial readout, or benefits from a significant real-world evidence publication, AI models will incorporate that information into their responses as their training data is updated, directly improving the competitor’s standing in comparative queries.
The second is that your own content strategy — publications, real-world evidence generation, patient education content, disease awareness campaigns — is simultaneously a scientific communication strategy and an AI influence strategy. Content that is indexed, replicated, and cited widely will shape AI model outputs. Content that lives behind a login wall, is published in limited-circulation journals, or is formatted in ways that resist AI indexing will not.
This doesn’t mean pharmaceutical companies should optimize their scientific communication for AI training data. It means they should understand that the two are now the same thing, and plan accordingly.
Regulatory Risk Monitoring: Building a Detection System
The FDA has not yet issued comprehensive guidance specifically addressing AI-generated drug information. But the agency has been clear in recent years that the information ecosystem around pharmaceutical products is a compliance consideration, and that manufacturers have obligations to monitor and respond to significant misinformation regardless of its source.
The practical regulatory risk taxonomy from AI drug information monitoring breaks down into four categories.
The first is factual inaccuracy in FDA-approved labeling language — wrong doses, wrong indications, wrong contraindications. This is the most straightforward category to detect and document, and the easiest to escalate through regulatory channels.
The second is comparative claims that violate fair balance requirements. When an AI describes a drug as ‘more effective’ or ‘safer’ than a competitor without the evidential basis that would be required in a promotional context, that language can circulate to millions of users without the disclaimers and caveats that would be mandatory in a pharmaceutical company’s own promotional materials.
The third is off-label recommendations, discussed above. The fourth is patient guidance that departs from prescribing information in ways that could affect clinical decision-making — for example, telling a patient that a drug can be safely discontinued without tapering when the label recommends a taper protocol.
None of these four categories can be detected by traditional pharmacovigilance systems. Adverse event reporting captures what happens to patients after they take drugs. AI monitoring captures what AI tells patients before they make decisions. The two are complements, not substitutes, and a complete regulatory monitoring architecture needs both.
Working With AI Companies on Content Accuracy
Several pharmaceutical companies have begun engaging directly with AI platform providers on drug information accuracy, with mixed results. The major AI companies have generally been receptive to factual corrections when they are clearly documented and involve patient safety risks. Persuading them to change subtle framing, competitive positioning, or emphasis patterns is harder, because those patterns are properties of model training rather than content that can be edited.
The more tractable approach for most companies is the indirect route: generating high-quality, well-indexed content that shapes training data for future model versions, while simultaneously using monitoring tools like DrugChatter to track whether deployed model versions are producing outputs that require escalation or formal FDA adverse finding reports.
Some manufacturers have also begun submitting structured drug information directly to AI platforms through emerging health data partnerships. Google’s MedPaLM team, Anthropic’s health-focused programs, and Microsoft’s partnership with Epic and Nuance create channels through which pharmaceutical companies can theoretically supply structured, labeled drug information that models can treat as authoritative. The commercial and legal frameworks for those relationships are still being defined, but they represent the most direct lever available for influencing AI drug knowledge at scale.
Voice of the Customer Through AI Query Analysis
The most underappreciated use of AI drug information monitoring is not regulatory risk detection or competitive tracking — it is voice of the customer research. AI platforms are receiving, in real time, the actual questions that patients and physicians have about drugs. Those questions are a direct, unfiltered window into patient and physician understanding, concerns, and decision-making frameworks.
Traditional patient insight research is slow, expensive, and subject to social desirability bias. Patients in a focus group don’t say ‘I’m afraid of this drug because I read something scary on Reddit.’ They say they want to discuss options with their physician. The questions they type into an AI system at midnight are a different kind of data — more honest, more specific, more indicative of actual decision barriers.
DrugChatter’s query analysis layer captures and categorizes the types of questions being asked about drugs across AI platforms, identifying themes, concerns, and knowledge gaps that brand and medical affairs teams can act on. If a significant fraction of patient queries about your drug involve a specific side effect concern, that concern needs to be addressed in patient education materials, prescriber communication, and potentially in label language if the signal is strong enough.
The same principle applies at the physician level. If physicians are asking AI systems about drug interactions your drug doesn’t have, that suggests a knowledge gap in your HCP communications. If they’re asking about dosing flexibility or off-label use patterns, that tells you something about how the drug is being used in practice that your Phase III trial design may not have captured.
Segmenting the Query Signal
Not all AI queries about a drug have the same strategic significance. A sophisticated monitoring program categorizes queries by intent — informational, comparative, decisional, safety-oriented — and by apparent user profile, using query language patterns to distinguish likely physician queries from likely patient queries.
A physician asking ‘what is the mechanism of action of drug X in treatment-resistant depression?’ is signaling something different from a patient asking ‘can I drink alcohol on drug X?’ Both signals matter, but they matter to different teams and require different responses.
DrugChatter’s query taxonomy enables this kind of segmentation, giving brand teams, medical affairs teams, and regulatory teams separate feeds of the AI intelligence most relevant to their functions. This matters practically because the organizational response to a factual error in physician-facing AI content is different from the response to misleading patient safety language — one goes through medical affairs and publication strategy, the other may go through regulatory affairs and potentially to the FDA.
The Content Strategy Implications
If AI model outputs are shaped by the content that enters their training data, and if that content is essentially the same as the content your scientific communication, patient education, and publications teams produce, then AI performance is a function of your existing content strategy — which means it can be systematically improved without creating a separate AI content function.
The specific interventions that improve AI drug intelligence accuracy and competitive positioning include:
Publishing structured, machine-readable real-world evidence that corrects gaps in the clinical trial literature. AI models are better at incorporating structured data than narrative prose, and real-world evidence published in peer-reviewed journals with clear, extractable data tables gets incorporated into AI training corpora more reliably than conference presentations or lay summaries.
Generating patient education content that directly and clearly addresses the questions patients actually ask. This sounds obvious. In practice, most pharmaceutical patient education content is written to satisfy regulatory review rather than to answer the questions that drive patient decision-making. AI query analysis reveals those questions explicitly; patient education content should be rebuilt around them.
Ensuring that disease state content, not just brand content, clearly establishes the therapeutic context in which your drug is appropriate. AI models answer symptom-level and condition-level queries more frequently than brand-name queries. If your disease awareness content clearly establishes the patient profile, treatment pathway, and clinical decision points that lead to your drug, the AI’s pathway-level responses will naturally position your drug more accurately.
Producing publication-quality head-to-head comparative data. In the absence of direct comparative trials, AI models fill the gap with whatever indirect comparison signals exist in their training data, which may include methodologically weak analyses or selective literature that favors a competitor. Direct comparative data, even from pragmatic trials or well-designed observational studies, gives AI models a stronger evidential anchor for competitive queries.
Building an AI Intelligence Function in Pharma
For most pharmaceutical companies, the organizational response to AI drug information monitoring is not yet defined. The monitoring falls between multiple existing functions — medical affairs, brand marketing, regulatory affairs, market access, patient advocacy — none of which owns it by default.
The companies moving fastest in this space are treating AI intelligence as a cross-functional capability, with a small dedicated team that pulls data from monitoring platforms like DrugChatter and distributes actionable intelligence to the appropriate functional owners. The dedicated team doesn’t produce patient education content or regulatory filings — it produces intelligence that enables other teams to act more effectively.
The resource requirement is not large relative to the scale of the problem. A monitoring program running structured query batteries across four to six AI platforms, covering a portfolio of ten to fifteen brands, can be operationalized with a two-person team and a platform subscription. The organizational challenge is less about resources than about incentives and ownership — ensuring that the intelligence gets routed to people who can act on it and who have the organizational motivation to do so.
The comparison to digital marketing is instructive. Twenty years ago, pharmaceutical companies didn’t have SEO functions, social media monitoring functions, or programmatic advertising expertise in-house. Those capabilities had to be built, often over the objection of traditional brand and regulatory teams who didn’t see digital channels as material. The companies that built those capabilities first captured lasting advantages in channel performance. The same dynamic is playing out now in AI.
What the Next 24 Months Will Bring
The AI pharmaceutical intelligence landscape will change substantially in the next two years, in ways that make early investment in monitoring capabilities more valuable, not less.
AI models are being updated and retrained more frequently. The interval between training data cutoffs is compressing from years to months for the major commercial models, which means the content environment for any given drug is shifting faster than it ever has. A monitoring program that checks AI outputs quarterly will miss changes that happen in weeks.
Agentic AI use is growing. The current paradigm — a user asks a question, an AI answers — is giving way to AI agents that proactively retrieve information, synthesize it, and take actions on the user’s behalf. An AI agent helping a patient manage a chronic condition will pull drug information repeatedly, in different contexts, without the patient necessarily knowing. The AI’s knowledge of the drug becomes a persistent factor in the management of that patient’s care.
AI is moving into clinical decision support at scale. Epic’s integration of AI into its clinical workflows, Nuance’s DAX system for physician documentation, and multiple health system deployments of conversational AI for patient triage are creating formal clinical touchpoints where AI drug knowledge directly influences prescribing. The stakes in those contexts are higher than in consumer AI use, and the regulatory attention will follow.
The FDA is watching. The agency’s Digital Health Center of Excellence has begun engaging with AI drug information questions, and multiple agency officials have indicated publicly that the regulatory framework for AI-generated health content is an active area of policy development. Companies that have built systematic monitoring programs will be better positioned to engage constructively with that regulatory process and to demonstrate due diligence if a specific AI drug information incident triggers agency inquiry.
Key Takeaways
AI models now function as a primary drug information channel for patients and physicians, fielding tens of millions of health queries per day across ChatGPT, Gemini, Copilot, Perplexity, and Claude. Most pharmaceutical companies have no systematic visibility into what those models say about their drugs.
The knowledge an AI model has about a drug is a weighted average of everything publicly written about it — clinical literature, patient forums, news coverage, adverse event reports, and promotional content. That weighting is not neutral, and it does not favor accuracy over volume. Drugs with longer commercial histories, more extensive publication records, and higher media salience tend to be described more confidently and favorably than newer drugs, regardless of relative clinical merit.
The four categories of AI drug information risk that warrant systematic monitoring are factual inaccuracy versus approved labeling, off-label recommendations, competitive framing bias, and patient safety guidance that departs from prescribing information. Traditional pharmacovigilance and brand monitoring systems capture none of these.
Share of AI voice — how frequently and how favorably your drug appears in AI-generated responses to relevant queries — is now a measurable brand metric with direct commercial consequences. Platforms like DrugChatter make it trackable at scale across multiple AI systems simultaneously.
AI query analysis is the most underutilized source of voice-of-customer intelligence in the pharmaceutical industry. The questions patients and physicians type into AI systems at the point of need are more honest and more decision-relevant than most primary market research.
The content strategy that improves AI drug intelligence performance is the same one that improves scientific communication, patient education, and HCP engagement generally — but it needs to be designed with AI indexability and training data dynamics in mind.
The regulatory and organizational infrastructure for AI drug information monitoring is still being built. The companies building it now will have meaningful advantages when the FDA moves from guidance development to enforcement, and when AI drug information incidents begin attracting the kind of attention that will make this a board-level issue.
FAQ
Q: Can a pharmaceutical company be held liable if an AI platform gives inaccurate information about their drug?
The legal framework is not settled, but the exposure is real. The FDA’s existing regulations require manufacturers to monitor the information environment around their products and take corrective action when significant misinformation is identified. Whether that obligation extends to AI-generated information is an open legal question, but the agency’s evolving guidance on digital health suggests it is moving in that direction. The more immediate risk is not FDA enforcement but product liability exposure if a patient suffers harm following an AI recommendation that the manufacturer knew, or should have known, was inaccurate.
Q: How often should pharmaceutical companies be running AI monitoring queries against their brands?
For drugs in competitive therapeutic areas or with complex safety profiles, weekly monitoring is the appropriate cadence. Major AI platforms update their models on irregular schedules, and a model update can shift outputs materially within days. Monthly monitoring is a minimum baseline for any commercially important brand. Quarterly monitoring, which is what most companies default to if they monitor at all, is too slow to detect changes in time to mount an effective response.
Q: Do different AI platforms give meaningfully different answers about the same drug?
Yes, consistently and significantly. The same query asked to ChatGPT, Gemini, Claude, and Perplexity can produce substantially different answers in terms of which drugs are mentioned first, what side effects are emphasized, and how comparative claims are framed. This variation reflects differences in training data composition, retrieval mechanisms, and model architecture between the platforms. Monitoring a single platform and extrapolating to the broader AI information environment is not adequate.
Q: What is the relationship between a drug’s AI intelligence profile and its performance in traditional social listening?
They are related but distinct. Social listening captures what users are saying about drugs in public forums and on social platforms. AI monitoring captures what AI systems are telling users about drugs. The two feed each other: social forum content is part of the training data that shapes AI outputs, and AI outputs increasingly shape what users search for and discuss in social forums. A complete monitoring program needs both, but the current gap is almost entirely in AI monitoring — social listening is mature and well-resourced in most pharma organizations, AI monitoring is not.
Q: How does DrugChatter’s monitoring differ from simply running manual queries on ChatGPT?
Manual queries by a brand team give you a snapshot — one drug, one platform, one point in time, with whatever prompts the team thought to use. DrugChatter runs structured, standardized query batteries across multiple platforms simultaneously, on a scheduled basis, covering the full range of query intents (informational, comparative, decisional, safety-oriented) at both the brand and category level. The outputs are scored, categorized, and trended over time, making it possible to detect changes, compare competitive positions, and prioritize response actions. It also generates structured documentation that can support regulatory submissions if an AI drug information incident requires a formal response.












")













