The pharmaceutical industry spent roughly $2.3 billion and 12 years, on average, bringing a single new molecular entity to market in 2023, according to the Tufts Center for the Study of Drug Development [1]. That figure gets cited in every biopharma boardroom as proof of the industry’s complexity, and it is accurate for the specific type of approval it describes. What the statistic systematically omits is the existence of a regulatory route that can cut those economics dramatically, one that the FDA has had on the books since 1984 and that the industry has only recently started using with real strategic sophistication.
The two approval pathways at the center of this analysis — 505(b)(1) and 505(b)(2) — govern the majority of new drug applications submitted to the U.S. Food and Drug Administration. The distinction between them is not a technicality. It determines capital requirements, development timelines, competitive positioning, intellectual property strategy, and ultimately the commercial viability of a product. Companies that understand this distinction at a structural level build drug development pipelines that generate returns. Companies that treat it as a regulatory compliance matter tend to struggle.
This article explains how the two pathways work, why they differ, and how sophisticated pharmaceutical companies use that difference to create defensible market positions with considerably less capital than traditional drug development demands.
Part One: The Legal Foundation
What the Hatch-Waxman Act Actually Did
The Drug Price Competition and Patent Term Restoration Act of 1984, universally known as the Hatch-Waxman Act, created the modern framework for pharmaceutical approvals in the United States. The Act’s primary stated purpose was to lower drug prices by making it easier for generic manufacturers to enter the market after a brand drug’s patents expired. It achieved that goal — the generic drug industry now accounts for approximately 90% of dispensed prescriptions in the United States [2].
What receives less attention is what Hatch-Waxman did for the brand-name side of the equation. The Act created Section 505(b) of the Federal Food, Drug, and Cosmetic Act, which defines three distinct pathways for new drug approval. Two of those pathways — 505(b)(1) and 505(b)(2) — apply to brand-name or innovative products and represent fundamentally different theories of how drug development investment should work.
The third pathway, 505(j), governs generic drug approvals through Abbreviated New Drug Applications (ANDAs) and operates on entirely different principles. This analysis focuses exclusively on the 505(b)(1) and 505(b)(2) routes.
The Text That Created the Pathway
Section 505(b)(2) of the Federal Food, Drug and Cosmetic Act states that an application may contain “investigations of safety and effectiveness… that were not conducted by or for the applicant and for which the applicant has not obtained a right of reference or use from the person by or for whom the investigations were conducted” [3].
That language is deliberately broad. It says, in practical terms, that a drug sponsor does not have to conduct every study from scratch if the FDA has already reviewed sufficient safety and effectiveness data on a related compound. The sponsor can rely on existing published literature, prior FDA findings on approved drugs, or a combination of both — supplemented by whatever new studies are necessary to demonstrate the specific differences in the new product.
The 505(b)(1) pathway, by contrast, contains no such permission. An application filed under 505(b)(1) must rest entirely on clinical investigations conducted by or for the applicant. Every piece of safety and efficacy evidence in the NDA must be original data the company either generated itself or has an explicit right of reference to use. This is the full clinical development model that produces the $2.3 billion average development cost.
FDA’s Regulatory Evolution on 505(b)(2)
The FDA did not immediately provide extensive guidance on how 505(b)(2) was supposed to work in practice. The statutory language existed from 1984, but meaningful utilization of the pathway came later, accelerated by a 1999 FDA guidance document titled “Applications Covered by Section 505(b)(2)” that clarified what types of products qualify and how the agency would treat reliance on existing data [4].
That guidance established that 505(b)(2) applies to products where the applicant wants to rely on existing findings to support approval but is seeking approval for something different from the listed drug — a different formulation, a different route of administration, a different dosage strength, a new indication, or a new combination. The guidance also clarified the relationship between the 505(b)(2) pathway and the patent certification requirements, which would become central to the litigation landscape that defines the pathway’s commercial environment.
Subsequent FDA guidances in 2019 and 2020 further refined the pathway’s mechanics, particularly around what types of published literature the agency would accept and how sponsors should structure their submissions when relying on data they didn’t generate [5]. The cumulative regulatory framework is now sophisticated enough that experienced regulatory counsel can predict, with reasonable confidence, what data packages the FDA will require for specific product types.
Part Two: The Mechanics of Each Pathway
How a 505(b)(1) Application Is Built
A full New Drug Application under 505(b)(1) is one of the most data-intensive regulatory submissions in any industry. The application is organized according to the Common Technical Document (CTD) format and typically runs to hundreds of thousands of pages across the five modules that cover administrative information, summaries, quality data, nonclinical study reports, and clinical study reports.
The clinical data package alone — Module 5 under the CTD structure — requires the applicant to have conducted its own Phase I, Phase II, and Phase III trials. For most drug candidates, Phase I establishes basic pharmacokinetics and safety in healthy volunteers. Phase II explores dose range and efficacy signals in the target patient population. Phase III delivers the definitive efficacy and safety evidence across a large patient population in controlled conditions.
This development process operates sequentially, with each phase dependent on data from the previous one. The FDA reviews Phase II results before a sponsor can define a Phase III protocol that the agency will consider adequate. Regulatory meetings — End-of-Phase 2 meetings, Pre-NDA meetings — punctuate the development timeline but do not abbreviate it. The process from IND filing to NDA submission, for a genuinely novel compound, routinely takes eight to twelve years.
The investment required tracks that timeline. Phase III trials for common indications can cost between $50 million and $500 million per trial, and a drug that fails in Phase III after a decade of development represents a complete write-off of everything spent to that point [6]. The 505(b)(1) model is a model of concentrated risk, which is why it is primarily the province of large pharmaceutical companies or well-funded biotech firms.
How a 505(b)(2) Application Is Built
A 505(b)(2) application uses the same CTD format and covers the same five modules, but the clinical data package is constructed differently. Rather than generating all safety and efficacy evidence de novo, the sponsor can draw on three distinct categories of existing data.
The first category is FDA’s previous findings of safety and/or effectiveness for an approved drug. When a sponsor references an approved listed drug — the Reference Listed Drug or RLD — the FDA’s prior review of that drug’s safety and efficacy becomes available for the sponsor to rely upon. The sponsor does not access the actual data from the original NDA (which remains confidential). Instead, the FDA’s published findings and the documented safety profile in the approved labeling constitute the evidential foundation the 505(b)(2) applicant builds upon.
The second category is published literature. Scientific papers, review articles, and peer-reviewed clinical data published in the public domain can support a 505(b)(2) application if they meet FDA’s standards for reliability and relevance. This matters most for active ingredients with long histories of use, where decades of published evidence may adequately characterize the safety profile without requiring new studies.
The third category is the applicant’s own studies. A 505(b)(2) application almost always includes original data, typically bridging studies, pharmacokinetic studies, or limited clinical trials that demonstrate how the new product’s differences from the RLD affect safety and efficacy. The key distinction from 505(b)(1) is that these studies do not need to recreate the entire safety and efficacy database from scratch.
The practical effect is that a 505(b)(2) sponsor may be able to bring a product to market with Phase I and Phase II data only — if the Phase III-equivalent evidence already exists for the referenced drug. For a reformulation of a well-understood active ingredient, the sponsor’s clinical burden might be limited to demonstrating that the formulation produces the expected pharmacokinetic profile and that any changes in exposure don’t introduce new safety concerns.
The Data Package Spectrum
The range of data packages within 505(b)(2) is wide, and that width is strategically important. At one end sits a product that differs from its RLD only in dosage form — say, a new extended-release version of an approved immediate-release tablet with the same active ingredient and same indication. Here, the applicant may need only pharmacokinetic bridging studies and perhaps a small safety study, with essentially all clinical efficacy support drawn from the RLD’s approved labeling.
At the other end sits a product with a new active ingredient that isn’t approved anywhere in the world but has significant published literature — perhaps a repurposed compound with decades of off-label use. The sponsor files under 505(b)(2) referencing published literature, but the FDA requires extensive Phase II and sometimes Phase III data because the existing evidence base isn’t sufficient to stand on its own.
Between these poles lies a spectrum of products that require different data packages depending on the nature and magnitude of the differences from what the FDA has already reviewed. Drug patent analysts at DrugPatentWatch regularly track these development programs, cataloguing what types of bridging data packages the FDA has accepted for specific product modifications — data that helps sponsors calibrate their regulatory strategy against precedents set by comparable approved products.
Patent Certifications and the Paragraph IV System
A 505(b)(2) applicant that references an approved drug must address the patents listed for that drug in the FDA’s Orange Book. This requirement — codified in 21 CFR 314.50(i) — produces one of the most commercially consequential features of the 505(b)(2) pathway.
The applicant must certify for each listed patent one of four things: that patent information hasn’t been submitted (Paragraph I); that the patent has expired (Paragraph II); that the patent will expire before the applicant wants to market (Paragraph III, triggering a wait until expiration); or that the patent is invalid or won’t be infringed by the applicant’s product (Paragraph IV).
A Paragraph IV certification is the one that creates the litigation mechanism. When a 505(b)(2) applicant files a Paragraph IV certification and the patent holder is notified, the patent holder has 45 days to sue for infringement. If they sue, an automatic 30-month stay of FDA approval takes effect, freezing the 505(b)(2) application while the patent dispute is litigated. This is the same mechanism that governs generic ANDA filers, and it creates the same litigation ecosystem around 505(b)(2) products.
The strategic implication is that 505(b)(2) applicants must understand the patent landscape of their reference drug as thoroughly as any other aspect of their development program. A failure to anticipate Paragraph IV litigation — or to structure the product in a way that avoids infringing valid patents — can add three years or more to time-to-market through the automatic stay mechanism.
Part Three: Intellectual Property Architecture
How 505(b)(1) Products Build IP Walls
A drug approved through 505(b)(1) typically carries multiple layers of intellectual property protection. The compound patent, protecting the new molecular entity itself, provides the most basic exclusivity — typically 20 years from filing, though the effective commercial patent life is much shorter due to the years consumed in clinical development. For many small molecule drugs, the compound patent expires before or shortly after the product reaches peak sales.
Savvy pharmaceutical companies therefore build patent estates around their NCEs that extend well beyond the compound patent. Formulation patents cover the specific way the drug is delivered. Method-of-use patents cover specific therapeutic applications. Process patents cover manufacturing methods. Combination patents cover the use of the compound with specific co-therapies. Polymorph patents cover specific crystalline forms of the active ingredient.
This strategy of secondary patenting has been extensively documented in academic literature and extensively criticized by generic manufacturers, patient advocates, and some academic economists who argue it extends monopoly pricing beyond what the innovation reward justifies [7]. The legal and ethical debate aside, the strategy works in commercial terms: it keeps generic competitors out of the market for years longer than the primary patent alone would.
The 505(b)(1) NDA holder also receives five years of New Chemical Entity (NCE) data exclusivity for a genuinely new molecular entity that has never been approved in the United States. During this five-year period, the FDA will not accept an ANDA or a 505(b)(2) application referencing the NCE. The practical effect is that the earliest a generic or 505(b)(2) competitor can even file is five years after approval, and with the Paragraph IV litigation process, the actual market entry of a competitor is routinely seven to twelve years after approval.
How 505(b)(2) Products Build IP Walls
A 505(b)(2) NDA holder receives three years of data exclusivity if the application contains new clinical investigations that are essential to approval — not the full five years available to NCE approvals, but still a meaningful protection window. During this three-year period, the FDA will not approve a generic product that relies on the 505(b)(2) holder’s clinical data.
This three-year exclusivity applies to each new approval that required new clinical investigations. A 505(b)(2) approval for a new formulation gets three years. A subsequent 505(b)(2) approval for a new indication of the same product gets another three years, but only for the new indication. Companies with sophisticated IP strategies stack these exclusivities deliberately, filing supplemental applications with new clinical data timed to extend the total exclusivity window.
505(b)(2) products can also use the full range of secondary patents available to any brand-name pharmaceutical product. Formulation patents, dosing regimen patents, and method-of-use patents can be listed in the Orange Book and enforced against subsequent 505(b)(2) or generic filers through the patent certification and litigation system. Many successful specialty pharma companies have built products with 505(b)(2) approvals that carried patent portfolios nearly as robust as those of NCE products, achieving effective market exclusivity windows that comfortably exceeded the initial three-year data exclusivity period.
The Evergreening Question
Critics of the Hatch-Waxman system — including academic researchers, generic industry representatives, and government price negotiators — point to both 505(b)(1) and 505(b)(2) as vehicles for “evergreening,” the practice of extending commercial exclusivity through incremental modifications that provide limited therapeutic improvement over existing drugs [8].
The criticism has different textures depending on the pathway. For 505(b)(1) products, the evergreening critique typically focuses on secondary patenting — the stacking of formulation and method-of-use patents on top of an expired compound patent. For 505(b)(2) products, the critique focuses on the pathway’s use to create barely-differentiated products that carry brand prices despite relying on safety and efficacy evidence generated by the original innovator.
These criticisms are legitimate in some specific cases. They are also overgeneralized in others. Many 505(b)(2) products deliver genuine clinical improvements — better tolerability profiles, more convenient dosing, pediatric formulations of adult drugs, or new combinations that improve patient adherence. The pathway is a tool, and like any tool, its value depends on how it is used.
The regulatory mechanism that’s supposed to screen for meaningful improvement is the FDA’s requirement that a 505(b)(2) applicant demonstrate not just that the product is safe and effective, but that it is safe and effective for its proposed use in a way that differs in a clinically relevant sense from what’s already on the market. In practice, the FDA does not require 505(b)(2) applicants to demonstrate superior efficacy — only that the product works for its claimed indication. The clinical differentiation argument happens in the marketplace, not at FDA.
Part Four: Development Economics
The Capital Model Under 505(b)(1)
The capital structure of a 505(b)(1) development program is straightforward and brutal. Investment is front-loaded, clinical risk is concentrated in Phase III, and the payoff — if it comes — arrives at approval, which is typically a decade or more after the initial investment decision.
A large pharmaceutical company financing a 505(b)(1) program through internal capital can absorb Phase III failures because its portfolio diversifies the risk. A biotech company relying on venture capital or public market financing faces a different calculus. Each clinical failure depletes the capital base, and clinical failures in Phase III are common — the average probability of transitioning from Phase III to approval is approximately 58% for all indications, and considerably lower for oncology, CNS, and other historically difficult therapeutic areas [9].
The venture capital community has responded to this risk profile with stage-gated financing structures that release capital in tranches conditional on clinical milestones. This structure limits the investor’s downside but also creates pressure on development teams to hit milestones on timelines that may not reflect the actual speed of good clinical science. The result, documented in multiple academic studies, is that Phase II studies are sometimes underpowered relative to what would be needed to confidently predict Phase III outcomes [10].
The cost of capital for 505(b)(1) programs reflects this risk. Biotech companies without approved products typically trade at substantial discounts to the expected net present value of their pipelines, because the market demands a risk premium for clinical failure, regulatory delay, and commercial execution uncertainty. The financing cost effectively adds to the total development cost even when it doesn’t appear in a simple accounting of clinical trial expenditures.
The Capital Model Under 505(b)(2)
505(b)(2) programs have a fundamentally different capital structure. Because the clinical data burden is lower — sometimes dramatically lower — the total investment required to reach NDA submission is smaller, and the timeline to that submission is shorter. Both effects improve the financial attractiveness of the investment.
The reduction in clinical investment is not uniform across 505(b)(2) programs. A product that requires only pharmacokinetic bridging studies might have a total development budget of $20 to $50 million, which is a fraction of even a modest Phase II-only 505(b)(1) program. A product that requires Phase II data plus a significant number of bridging studies might spend $100 to $200 million. The range is wide, but the upper end of the 505(b)(2) range is typically still well below the lower end of a conventional Phase III trial budget. <blockquote> “Specialty pharmaceutical companies using the 505(b)(2) pathway spend, on average, 40 to 60 percent less on clinical development than companies pursuing full 505(b)(1) NDAs for comparable therapeutic areas,” according to analysis published in the Journal of Clinical Pharmacology [11]. </blockquote>
The shorter timeline compounds the capital efficiency advantage. A development program that takes four years instead of twelve consumes four years of operating costs rather than twelve, and the cash flows from product sales begin arriving eight years earlier. When discounted back to present value, this timing difference is often larger than the direct cost savings from reduced clinical trials.
The risk profile is also different in ways that matter to investors. A 505(b)(2) program referencing a drug with a decades-long safety history carries lower clinical risk than an NCE program entering Phase I with a compound that has never been in a human body. The probability of regulatory approval — conditional on filing — is higher for well-structured 505(b)(2) applications than for NCE 505(b)(1) applications, because the FDA has already reviewed and accepted the core safety and efficacy evidence being relied upon.
Return on Investment Comparisons
Comparing ROI across the two pathways requires careful control for therapeutic area, market size, and IP durability. These variables dominate the return calculation. A 505(b)(1) NCE in a large oncology indication with strong patents can generate far higher returns than a 505(b)(2) reformulation in a crowded cardiovascular space with weak IP.
That said, general patterns are observable. Research by the Deloitte Centre for Health Solutions tracking 505(b)(2) products against NCE products over multiple years found that the 505(b)(2) products achieved break-even faster and generated positive ROI at lower peak sales levels — a direct consequence of the lower investment base [12]. The risk-adjusted return for a median 505(b)(2) program outperforms a median 505(b)(1) program in most analyses, largely because the denominator (capital invested) is smaller and the probability of approval (conditional on filing) is higher.
This risk-adjusted return advantage does not hold in all scenarios. When a 505(b)(2) product faces immediate generic competition because it carries weak IP and a small market, the commercial window can be too short to recoup even the reduced development investment. The IP architecture matters as much as the regulatory pathway in determining commercial outcomes.
Part Five: The Patent Landscape
Reading the Orange Book for 505(b)(2) Strategy
The FDA’s Orange Book — formally titled “Approved Drug Products with Therapeutic Equivalence Evaluations” — is the central database for understanding the IP landscape around any drug product. It lists patents that the NDA holder certified as covering the product, along with their expiration dates and any market exclusivity periods.
For a 505(b)(2) sponsor planning to reference a specific listed drug, Orange Book analysis is a prerequisite. The analysis needs to cover three questions: which patents are listed, when they expire, and whether the proposed 505(b)(2) product would infringe them.
The first two questions are straightforward — the Orange Book provides the information directly. The third is a legal analysis that requires patent counsel to review the claims of each listed patent and assess whether the 505(b)(2) product falls within those claims. This analysis has to happen before the applicant determines the Paragraph certification it will file, because the certification decision determines whether the 30-month automatic stay is triggered.
DrugPatentWatch provides comprehensive patent expiration and listing data that supplements the Orange Book, including tracking of patent term extensions, pediatric exclusivities, and litigation outcomes that affect the effective exclusivity timeline. For companies evaluating the competitive timing of a 505(b)(2) application, this data allows precise modeling of when regulatory approval could become final — and when generic competition is likely to follow.
Patent Carve-Outs and Section viii Statements
One tool available to 505(b)(2) applicants who want to avoid Paragraph IV litigation is the Section viii statement — a certification that the applicant’s label will not include the use covered by a specific Orange Book patent. If the 505(b)(2) product is seeking approval only for indications not covered by a method-of-use patent, the sponsor can carve that use out of its label entirely and submit a Section viii statement rather than a Paragraph IV certification.
This approach avoids the 30-month stay for the method-of-use patent, which means the applicant can potentially receive approval before that patent expires, as long as no other unexpired patents trigger a Paragraph IV stay. The carved-out indication is simply absent from the label; physicians can still prescribe the drug off-label for that use, but the company cannot promote it.
Section viii statements create their own strategic complications. Regulatory counsel must be certain that the 505(b)(2) product’s label doesn’t directly reference or rely on the carved-out use in any way. The FDA’s evaluation of whether a carve-out is permissible involves detailed review of the proposed labeling, and carve-outs are rejected when the label cannot be rendered safe and informative without including language that references the patented use.
The Pediatric Exclusivity Wrinkle
Pediatric exclusivity adds six months to any existing patent or data exclusivity period when an NDA holder conducts studies in pediatric populations requested by the FDA under the Pediatric Research Equity Act or voluntarily under the Best Pharmaceuticals for Children Act [13]. This extension applies to all patents listed in the Orange Book for the product, not just the patent under which the studies were conducted.
For 505(b)(2) sponsors timing their market entry, pediatric exclusivity on the reference drug can extend the effective exclusivity window in ways that don’t appear in a basic patent expiration analysis. A patent that appears to expire in three years may carry a six-month pediatric exclusivity that effectively extends the block to three and a half years. Tracking these exclusivities accurately requires monitoring FDA’s list of pediatric exclusivity grants, which DrugPatentWatch maintains as part of its ongoing patent landscape analysis.
Patent Term Extension Under Hatch-Waxman
Hatch-Waxman’s original patent restoration provisions allow NDA holders to extend the term of one patent by up to five years to compensate for the time spent in FDA review. The extension cannot exceed 14 years of post-approval patent life, and only one patent per product receives the extension [14].
For 505(b)(1) NCE products, patent term extensions are often essential to maintaining commercial exclusivity long enough to recoup development investment. The compound patent, filed before clinical development begins, may have only a few years of term remaining when the product finally receives FDA approval. The extension — while capped — can mean the difference between a few years of market exclusivity and a decade.
For 505(b)(2) products, patent term extension is available but less frequently pursued, because the product often relies on a compound patent held by the original innovator rather than by the 505(b)(2) sponsor. The 505(b)(2) sponsor’s patents are typically formulation or method-of-use patents, for which patent term extension is available but less commonly granted — because FDA review time for a 505(b)(2) application is typically shorter than for an NCE, leaving less patent life to compensate for.
Part Six: Regulatory Strategy in Practice
Choosing the Right Pathway
The decision between 505(b)(1) and 505(b)(2) is not simply a matter of choosing the cheaper option. It starts with the product itself. If the sponsor is developing a genuinely novel compound — a new molecular entity with a mechanism of action that has never been clinically evaluated — 505(b)(2) is typically not an option. There is no existing FDA review to rely upon, no listed drug with a relevant safety database, and no published literature that adequately characterizes the compound’s clinical profile. The development must proceed under 505(b)(1).
If, however, the sponsor is working with a known active ingredient — approved or in the published literature — 505(b)(2) becomes viable, and the question shifts to whether the differences between the proposed product and the reference create clinical uncertainties that require significant new trials.
The FDA itself provides guidance on how to approach this question through its guidance documents and the Type B meeting process. A Pre-IND meeting (Type B meeting) with the FDA, in which the sponsor presents its proposed product and development plan, allows the agency to identify what data it will require before accepting the 505(b)(2) application. This interaction is invaluable because it converts regulatory uncertainty into a defined clinical work plan. Sponsors who skip this meeting to save time almost invariably spend more time later addressing deficiencies the FDA would have flagged upfront.
Bridging Study Design
The bridging study is the structural centerpiece of most 505(b)(2) applications. A bridging study establishes, through head-to-head comparison with the reference drug, that the 505(b)(2) product has a pharmacokinetic profile consistent with the expected safety and efficacy of the active ingredient at the proposed dose in the proposed formulation.
For a solid oral dosage form seeking to establish bioequivalence in terms of rate and extent of absorption, the bridging study design is well-established. For more complex products — depot injectables, transdermal systems, inhaled formulations — the bridging criteria are more complex and often require sponsor-FDA dialogue to define acceptable endpoints.
The key variable in bridging study design is the variability of the pharmacokinetic parameters being measured. High within-subject variability in Cmax or AUC makes it difficult to meet the standard 80-125% bioequivalence window with a reasonably sized study. Sponsors faced with highly variable drugs must either use reference-scaled average bioequivalence approaches — which FDA has accepted for specific high-variability drugs — or accept larger studies with more subjects to achieve adequate statistical power.
Labeling Negotiations
Labeling is where 505(b)(2) applications often generate the most regulatory complexity. The 505(b)(2) product’s label must be consistent with the approved labeling of the reference drug for all indications and uses that rely on the reference drug’s data. Where the 505(b)(2) product differs — in formulation, dosing, population, or specific indication — the label must reflect those differences, supported by the applicant’s own data.
Carve-outs of patented uses complicate this process because the FDA must agree that the carved-out use can be removed from the label without making the label incomplete or misleading. For products where the carved-out use is central to safe prescribing — because dosing adjustments or contraindications are tied to that use — the FDA may require that some reference to the use remain, which could compromise the carve-out strategy.
505(b)(2) sponsors should budget substantial time and regulatory resources for labeling negotiations. Complete Response Letters from the FDA in the context of 505(b)(2) applications frequently include labeling-related deficiencies, and these deficiencies can add months to the approval timeline even after the clinical data package has been accepted as adequate.
FDA’s Review Division Structure and 505(b)(2)
The FDA’s review divisions matter to 505(b)(2) strategy in ways that are underappreciated. Different review divisions within the FDA’s Center for Drug Evaluation and Research have different cultures around 505(b)(2) applications, different templates for what bridging data packages they expect, and different speeds of review.
The Division of Neuroscience, for example, has historically been cautious about 505(b)(2) applications for CNS drugs, often requiring Phase II data even when a sponsor believed published literature was sufficient. The Division of Dermatology and Dentistry has more extensive experience with topical formulation 505(b)(2) applications and clearer expectations about what bridging data is needed for different product categories.
Experienced regulatory consultants spend years mapping these divisional tendencies and building relationships with division staff. This institutional knowledge about how specific FDA reviewers interpret the 505(b)(2) data requirements is a genuine competitive advantage for companies with experienced regulatory teams, and it’s a knowledge gap that can produce expensive surprises for companies relying on generic regulatory advice.
Part Seven: Market Dynamics and Competitive Strategy
The Specialty Pharma Business Model
The 505(b)(2) pathway has been the foundation of the specialty pharmaceutical business model for the past two decades. Companies like Medicis Pharmaceutical, Warner Chilcott, Noven Pharmaceuticals, and Assertio Therapeutics built significant commercial franchises around 505(b)(2) products — reformulations, new dosage forms, and new delivery systems for known active ingredients targeting markets where the original innovator had either left the field or was inattentive to formulation innovation.
The business model’s appeal is structural. By reducing the clinical development investment relative to NCE development, specialty pharma companies can achieve positive ROI at much lower peak sales levels. A product generating $50 million in annual revenues might not be commercially interesting to a large pharma company with a $500 million development cost basis, but the same product at the same sales level represents excellent economics for a specialty pharma company with a $30 million development cost basis.
This economic structure also makes 505(b)(2) products attractive as acquisition targets for larger pharma companies looking to diversify revenue without taking on the full development risk of NCE programs. Multiple pharmaceutical M&A transactions over the past decade have involved acquiring companies built on 505(b)(2) portfolios, with buyers paying acquisition premiums that reflected the lower-risk earnings streams.
Therapeutic Areas Where 505(b)(2) Dominates
The 505(b)(2) pathway dominates particular therapeutic areas where formulation innovation is commercially valuable and the underlying science is well-established. Pain management is one clear example: extended-release formulations of analgesics, abuse-deterrent formulations, and transdermal delivery systems for opioid and non-opioid analgesics have all been approved through 505(b)(2) routes. The commercial rationale is patient convenience and improved tolerability, both of which can support premium pricing against older formulations.
Dermatology is another area with extensive 505(b)(2) activity. Topical formulations involve complex interactions between active ingredient concentration, vehicle composition, skin penetration, and local tolerability. Small changes in formulation can produce meaningful differences in patient experience, and the clinical pathway for demonstrating these differences is relatively well-defined — typically vasoconstrictor assays for topical steroids or comparative clinical studies with a defined primary endpoint.
Psychiatry has seen 505(b)(2) applications for long-acting injectables of antipsychotic drugs, where the clinical rationale is improving medication adherence in a population with documented adherence challenges. The FDA has generally been receptive to these applications when the sponsor provides adequate PK bridging data and a demonstration that the long-acting formulation achieves therapeutic drug levels comparable to the approved oral formulation.
Women’s health, CNS, and rare disease have also produced significant 505(b)(2) approvals, with the pathway being used for new indications, age-appropriate formulations (particularly pediatric), and combination products that integrate previously separate therapies.
The Authorized Generic Threat
A strategic risk specific to 505(b)(2) products is the authorized generic. When a 505(b)(2) product’s exclusive marketing period ends — either at data exclusivity expiration or when a generic/subsequent 505(b)(2) competitor achieves approval — the original 505(b)(2) NDA holder can respond by authorizing a generic version of its own product.
The authorized generic captures revenues that would otherwise go to the competing generic and creates price competition that may limit the subsequent entrant’s market share. For 505(b)(2) products with limited patent protection, the authorized generic strategy is often more commercially effective than litigation, because it accepts price erosion while maintaining volume.
This means that subsequent 505(b)(2) entrants targeting the same reformulated product as an existing 505(b)(2) face a dual competitive threat: they must overcome any remaining IP protections held by the incumbent, and they must model their commercial projections assuming the incumbent will respond to their entry with an authorized generic or significant price reduction.
When 505(b)(2) Fails Commercially
Not all 505(b)(2) products succeed in the marketplace, and understanding the failure modes is as important as understanding the success cases. The most common commercial failure mode for 505(b)(2) products is insufficient differentiation relative to the available alternatives.
A product that offers only marginal improvements in bioavailability or tolerability — improvements that don’t translate into meaningful differences in patient outcomes or physician prescribing preferences — may receive FDA approval but fail to justify a price premium over existing alternatives. Without a price premium, the revenue model collapses, and the product can’t generate returns adequate to justify even the reduced 505(b)(2) development investment.
The payer environment has intensified this dynamic. Pharmacy benefit managers and insurance formulary committees increasingly scrutinize new product listings, demanding evidence not just of safety and efficacy but of clinical superiority over existing alternatives or at least cost-effectiveness parity. A 505(b)(2) product that can’t meet that bar will be placed on unfavorable formulary tiers that limit patient access and suppress sales.
Companies that succeed commercially with 505(b)(2) products typically conduct thorough market research before committing to development — not just on clinical need but on payer willingness to cover the product at a price that makes the investment worthwhile. This commercial due diligence is as important as regulatory strategy and, in well-managed specialty pharma companies, happens before the development program is finalized.
Part Eight: The Litigation Ecosystem
Paragraph IV Certifications and the 30-Month Stay
The litigation environment around 505(b)(2) mirrors, in most structural respects, the generic ANDA litigation environment that has been thoroughly documented and analyzed since Hatch-Waxman’s passage. When a 505(b)(2) applicant files Paragraph IV certifications against Orange Book-listed patents, the 45-day window for the patent holder to file suit creates a predictable trigger for litigation.
The number of 505(b)(2)-related Paragraph IV patent cases has grown substantially over the past decade. FDA’s Orange Book data shows increasing numbers of 505(b)(2) applications with Paragraph IV certifications each year, and the legal infrastructure — specialized IP counsel, litigation finance companies that fund patent disputes in exchange for a share of settlement proceeds, and judges in the District of Delaware and District of New Jersey with extensive pharmaceutical patent experience — is well-developed to process these cases [15].
The automatic 30-month stay, which pauses FDA approval of the 505(b)(2) application while litigation proceeds, is designed to protect patent holders from premature market entry before their IP rights are adjudicated. In practice, most Paragraph IV cases settle before final judgment, often with license agreements that allow the 505(b)(2) applicant to launch on a defined date that is earlier than the patent expiration but later than their preferred launch date.
These settlements have attracted regulatory scrutiny. “Reverse payment” settlements — in which the patent holder pays the applicant to delay market entry — were the subject of the U.S. Supreme Court’s 2013 FTC v. Actavis decision, which held that such settlements can be anticompetitive under antitrust law [16]. While Actavis directly addressed generic ANDA settlements, its reasoning applies to 505(b)(2) settlements as well, and the FTC has indicated it monitors 505(b)(2) settlement agreements for compliance with the same antitrust principles.
Building Litigation-Proof 505(b)(2) Products
Companies that approach 505(b)(2) development with litigation risk in mind structure their products to minimize Paragraph IV exposure from the outset. This means conducting freedom-to-operate analysis early in development — before committing to a specific formulation or delivery system — to identify which formulation approaches avoid infringement of Orange Book-listed patents.
Freedom-to-operate analysis for a 505(b)(2) product starts with identifying all Orange Book patents for the reference drug and all potential reference drugs. It then involves a patent claim-by-claim analysis to assess whether a given product design falls within the scope of any listed claim. Where infringement is possible, the design is modified to design around the patent claim, or counsel provides a non-infringement opinion that gives the company a reasonable basis for a Paragraph IV certification.
The earlier this analysis happens, the less expensive it is. A freedom-to-operate analysis conducted at the formulation selection stage can influence the formulation design before significant development investment is made. The same analysis conducted after a product is fully developed and manufacturing processes are locked may identify infringement risks that can’t be designed around without starting formulation development over.
Inter Partes Review as a 505(b)(2) Defense
The America Invents Act of 2011 created the Inter Partes Review (IPR) process at the Patent Trial and Appeal Board (PTAB), which allows challengers to contest patent validity through an administrative proceeding that is faster and less expensive than district court litigation [17]. 505(b)(2) applicants facing Orange Book patent infringement suits have increasingly used IPR petitions as a parallel track to Paragraph IV litigation.
The IPR advantage is that it can invalidate patents on prior art or obviousness grounds without requiring the 505(b)(2) applicant to prove non-infringement in district court. If the PTAB invalidates the blocking patent, the automatic 30-month stay may dissolve, and the 505(b)(2) application can proceed to approval. Even if the PTAB doesn’t invalidate the patent outright, IPR proceedings often lead to narrowed claims that the 505(b)(2) product doesn’t infringe — effectively achieving freedom to operate through claim amendment.
The combination of Paragraph IV litigation in district court and parallel IPR proceedings at the PTAB has become standard practice for sophisticated 505(b)(2) litigants. The dual-track approach creates settlement pressure on patent holders who face the risk of having their patents invalidated at PTAB while simultaneously defending them in district court — a resource-intensive and strategically uncomfortable position.
Part Nine: Regulatory and Policy Trends
FDA’s Increasing 505(b)(2) Approval Rate
The FDA’s approval rate for 505(b)(2) applications has risen steadily over the past fifteen years, reflecting several concurrent trends. The FDA has gained extensive experience reviewing 505(b)(2) applications and has developed clearer internal standards for what data packages are adequate for different product types. The agency has also published multiple guidances that have reduced the uncertainty around specific aspects of 505(b)(2) development, including guidance on bioequivalence for complex drug products, extended-release formulations, and locally acting drug products.
The Prescription Drug User Fee Act (PDUFA) commitments — the performance goals the FDA agrees to in exchange for industry user fees — have shortened review timelines for all NDA types, including 505(b)(2). Standard PDUFA review goals require FDA to complete review of a standard 505(b)(2) application within 12 months of filing, with a 6-month goal for priority applications. These timelines, while not always met, have substantially shortened the time between NDA submission and approval decision compared to the pre-PDUFA era.
Looking at the data: in fiscal year 2022, the FDA approved 37 original NDAs under 505(b)(2), representing approximately 40% of all original NDA approvals that year. The pathway has become a mainstream regulatory route, not a specialty niche [18].
The Emerging Complex Drug Product Landscape
Regulatory policy is increasingly focused on what FDA terms “complex drug products” — products where the relationship between the drug’s physicochemical properties and its clinical performance is not fully characterized by simple pharmacokinetic parameters. Complex drug products include complex mixtures (like certain peptides and proteins), complex formulations (like liposomal drugs or PEGylated molecules), and complex delivery systems (like metered-dose inhalers and drug-device combination products).
These complex products represent the frontier of 505(b)(2) development. The pathway is viable for complex drugs when the active ingredient is known and the question is whether the new formulation performs comparably to the reference product. But demonstrating comparability for a liposomal formulation requires a much more sophisticated analysis than a simple PK bridging study — it may involve in vitro dissolution testing, tissue distribution studies, and bioequivalence methods that are still evolving.
The FDA’s Suitability Petition process, used to confirm that a specific product can be filed as a 505(b)(2), is particularly important for complex drug products because the answer to “is this a 505(b)(2)?” isn’t always obvious. Several FDA guidances, including those on complex active ingredients and locally acting drugs, have clarified the agency’s thinking on specific product types, but many complex drug categories still require sponsor-FDA dialogue to establish the appropriate regulatory pathway.
The Biosimilars Parallel
The 505(b)(2) framework for small molecule drugs has an analog in the biologics space — the Biologics Price Competition and Innovation Act (BPCIA) biosimilar pathway. Like 505(b)(2), the BPCIA pathway allows biosimilar sponsors to rely on FDA’s prior finding of safety and effectiveness for the reference biological product (RBP), supplemented by analytical similarity data and, in some cases, clinical studies.
The parallel is imperfect — biologics have different scientific complexity and different exclusivity structures than small molecules — but the underlying regulatory logic is similar. Where the science of a biologic is sufficiently well-characterized that new clinical data can be limited to demonstrating similarity rather than establishing de novo safety and efficacy, the development burden can be reduced through reliance on prior findings.
The policy debates around biosimilars — how much interchangeability should be granted, what extrapolation of indications is appropriate, how to handle reference product patents — echo debates that played out in the small molecule 505(b)(2) context years earlier. Watching how courts and regulators resolve biosimilar questions provides useful predictive signal for how similar questions might be resolved if they arise in the 505(b)(2) context.
The IRA’s Effect on 505(b)(2) Economics
The Inflation Reduction Act of 2022 introduced Medicare drug price negotiation for a defined set of high-expenditure drugs, with the negotiated prices taking effect progressively starting in 2026 [19]. The IRA’s provisions are structured around drug age — small molecule drugs become eligible for negotiation as early as seven years after approval, biologics at eleven years.
This timeline interacts with 505(b)(2) products in ways that could reshape development economics. A 505(b)(2) product’s five-year NCE exclusivity (if applicable) or three-year data exclusivity period may expire before the IRA negotiation timeline kicks in, but the negotiation timeline gives brand-name manufacturers considerably less certainty about long-term revenue at current prices.
For 505(b)(2) sponsors whose products are expected to generate significant Medicare expenditures, the IRA creates new financial modeling requirements. Products that would previously have been projected to maintain high prices through extended patent protection now must be modeled with negotiated price scenarios in the later years of their commercial life. This shortens the effective commercial window for premium pricing and reduces the expected NPV of some 505(b)(2) programs at the margin.
The IRA effect is most pronounced for high-priced specialty products targeting elderly populations with significant Medicare coverage — exactly the population most 505(b)(2) sponsors have historically targeted. The pathway’s economics remain attractive in absolute terms, but the regulatory and pricing environment is less favorable than it was five years ago.
Part Ten: Case Studies
Apriso and the 505(b)(2) Reformulation Model
Salix Pharmaceuticals’ Apriso (mesalamine extended-release capsules) received FDA approval in 2008 through a 505(b)(2) NDA. Mesalamine — an aminosalicylate used to treat ulcerative colitis — had been available in multiple formulations for decades, including suppositories, enemas, and various oral dosage forms. Salix’s innovation was a once-daily extended-release formulation using a proprietary Multi-Matrix system that released mesalamine throughout the colon with improved distribution compared to earlier oral formulations.
The clinical development program for Apriso relied on the established safety and efficacy record of mesalamine documented in prior approvals and published literature, supplemented by Salix’s own Phase III clinical trials demonstrating efficacy and tolerability of the specific Apriso formulation. The 505(b)(2) pathway allowed Salix to reference the existing mesalamine safety database rather than repeating safety characterization from scratch, while the new Phase III data established the specific formulation’s efficacy [20].
Apriso achieved peak annual revenues exceeding $200 million before generic competition and subsequent biosimilar-like entrants entered the market. The commercial success reflected both genuine clinical utility — once-daily dosing improved patient adherence in a chronic disease condition — and effective IP protection through formulation patents.
Concerta and the Abuse-Deterrent Reformulation Strategy
OROS methylphenidate (Concerta) illustrates a different 505(b)(2) dimension. Methylphenidate had been used in ADHD treatment since the 1950s. Alza Corporation’s OROS delivery system, licensed to McNeil Consumer Healthcare, created an extended-release formulation with a distinctive pharmacokinetic profile that was both clinically useful and commercially valuable.
The Concerta story led to a subsequent generation of 505(b)(2) applications for generic versions of the OROS system that the FDA eventually determined were not therapeutically equivalent to the brand product — a finding that highlighted the complexity of demonstrating bioequivalence for sophisticated controlled-release mechanisms and led the agency to clarify its bioequivalence standards for complex oral formulations [21].
The broader lesson is that 505(b)(2) products built on novel delivery mechanisms can achieve greater IP durability than products built on simple formulation modifications, because the bioequivalence standard for complex delivery systems is harder for subsequent entrants to satisfy.
Vimovo: The Combination Product Example
Vimovo (naproxen and esomeprazole) received FDA approval in 2010 through a 505(b)(2) NDA. The product combined an NSAID with a proton pump inhibitor in a single fixed-dose combination tablet, designed to treat arthritis pain while reducing the gastrointestinal risk associated with chronic NSAID use.
Both active ingredients — naproxen and esomeprazole — were individually approved drugs with extensive safety records. The 505(b)(2) application relied on that existing data to characterize the safety of each component and supplemented it with new clinical trials demonstrating the combination’s efficacy in reducing NSAID-associated gastric ulcers while maintaining naproxen’s anti-inflammatory efficacy [22].
Vimovo’s commercial model depended on physicians prescribing a convenient single tablet rather than two separate medications. The product commanded a significant premium over the cost of purchasing naproxen and esomeprazole generics separately, a pricing strategy that attracted payer scrutiny and ultimately limited the product’s commercial reach.
The Vimovo case illustrates both the potential and the limitation of combination product 505(b)(2) strategies. The regulatory pathway is generally clear when combining two approved products. The commercial challenge is convincing payers that the convenience premium justifies the cost differential, particularly when the individual generic components are inexpensive and widely available.
Probuphine and the Implant Innovation
Probuphine — a subdermal buprenorphine implant approved by the FDA in 2016 — represents one of the more ambitious 505(b)(2) applications in recent memory. Buprenorphine for opioid use disorder treatment was well-established in sublingual formulations (Suboxone, Subutex). Braeburn Pharmaceuticals developed a 6-month subdermal implant that delivered a continuous low-dose release of buprenorphine, addressing the adherence challenges inherent in daily or twice-daily sublingual dosing.
The 505(b)(2) application relied on the extensive buprenorphine safety database from sublingual formulations while providing new pharmacokinetic and clinical data for the implant delivery system. The clinical data package required Phase III trials demonstrating the implant’s efficacy in maintaining opioid abstinence — a more extensive clinical program than simpler reformulation 505(b)(2) applications, but still considerably smaller than would have been required for a new molecular entity addressing opioid use disorder [23].
Probuphine’s approval and subsequent limited commercial success illustrate the gap that can exist between regulatory accomplishment and commercial viability. Despite genuine clinical utility in a severe public health problem, the product’s complex insertion and removal procedures limited uptake to addiction medicine specialists willing to undergo required REMS training, constraining the addressable prescriber pool.
Part Eleven: Data Tools and Competitive Intelligence
Patent Expiration Analysis for 505(b)(2) Planning
Competitive intelligence is central to 505(b)(2) strategy. The decision to develop a 505(b)(2) product targeting a specific reference drug depends critically on accurate understanding of when existing patents expire, what exclusivities protect the reference drug, and when competitive entry becomes legally possible.
DrugPatentWatch is a primary data resource for this analysis, providing patent expiration dates, Orange Book listings, exclusivity expiration dates, and patent challenge histories for approved drugs. Companies building 505(b)(2) development pipelines use the platform to identify drugs whose formulation patents are approaching expiration — creating windows in which a 505(b)(2) entrant could achieve market entry without triggering a 30-month stay from Paragraph IV litigation.
The analysis requires layering multiple data streams. Patent expiration dates from the Orange Book are the starting point, but they need to be cross-referenced with pediatric exclusivity grants that can extend effective exclusivity beyond the basic patent term, with any pending patent term extension applications, and with the outcomes of any prior Paragraph IV litigation that may have settled on terms creating contractual market exclusivity beyond the patent expiration date.
Tracking 505(b)(2) Filing Activity
The FDA’s public database of pending NDA applications — visible through the FDA’s Drug Approvals and Databases section — does not comprehensively reveal the universe of pending 505(b)(2) filings before they are approved or publicly disclosed. But regulatory intelligence services, including DrugPatentWatch’s application tracking capabilities, can identify Orange Book patent challenges and Paragraph IV litigation filings that signal active 505(b)(2) development programs targeting specific reference drugs.
When a company files a Paragraph IV certification and notifies the patent holder, the patent holder’s decision to file suit (or not) becomes a matter of court record, creating public visibility into the 505(b)(2) applicant’s existence and target. This signal, while imperfect, provides meaningful competitive intelligence to other companies evaluating the same space.
Understanding the competitive landscape for a 505(b)(2) target is important because multiple companies can simultaneously develop 505(b)(2) products targeting the same reference drug. Unlike the ANDA context — where the first generic filer receives 180-day exclusivity — there is no first-filer exclusivity for 505(b)(2) applications. Multiple 505(b)(2) products for the same therapeutic space can be approved simultaneously, creating price competition that erodes the premium pricing model that justifies 505(b)(2) development in the first place.
Post-Approval Monitoring
After a 505(b)(2) product is approved and commercialized, ongoing competitive intelligence remains important. The FDA’s approval of a competitor’s 505(b)(2) application referencing the same drug — or approval of a generic ANDA for the 505(b)(2) holder’s product — changes the competitive landscape in ways that affect pricing strategy, sales force allocation, and marketing investment.
DrugPatentWatch’s approval tracking allows companies to monitor the competitive pipeline for their marketed 505(b)(2) products with reasonable granularity, including identifying when competitors achieve patent certifications that could signal imminent generic competition. This information is useful not just for commercial strategy but for financial planning — accurately timing expected generic entry is essential for financial modeling and investor communication.
Part Twelve: The Future of the 505(b)(2) Pathway
Digital Health and Drug-Device Combinations
Drug-device combination products represent one of the fastest-growing areas of pharmaceutical development and create some of the most complex 505(b)(2) questions. An inhaled dry powder formulation of an approved drug, delivered via a new proprietary inhaler device, requires approval of both the drug component and the device component. If the drug component is approved via a 505(b)(2) referencing a prior inhaled drug formulation, the device must be evaluated as a component of the combination product under FDA’s Office of Combination Products jurisdiction.
The regulatory pathway for these products is genuinely complex, with different FDA centers (CDER for the drug, CDRH for the device) having concurrent jurisdiction over different aspects of the product. Companies navigating this space benefit from early engagement with both centers and from retaining regulatory counsel with specific combination product experience — which is distinct from experience in either drug or device regulation alone.
Digital health integration adds another dimension. Software-based dosing systems, companion applications that track adherence, and connected delivery devices create regulatory questions about which components of the overall system require FDA clearance or approval and what evidence must support each component. The FDA’s Digital Health Center of Excellence has been working to clarify these pathways, but the regulatory framework is still evolving.
Personalized Medicine and 505(b)(2)
Precision medicine — treatments tailored to individual patients based on genetic markers, biomarker profiles, or other individualized characteristics — might seem incompatible with the 505(b)(2) model, which emphasizes reliance on prior population-level data. In fact, the two concepts have an interesting intersection.
A drug with an approved indication for a broad patient population may be known from published literature or post-marketing data to be particularly effective — or particularly toxic — in a genetically defined subpopulation. A 505(b)(2) application seeking approval for the use of that drug specifically in that genetically defined subpopulation, with a label that includes companion diagnostic requirements, could rely on the existing safety database for the general population while supplementing it with new clinical data characterizing outcomes specifically in the targeted subpopulation.
This structure effectively narrows the approved indication to a patient subset while using the broad safety database already reviewed by the FDA. The commercial logic could work in orphan drug contexts, where the patient population is small enough that the three-year data exclusivity and potential orphan drug designation protections combine to create a defensible commercial position.
The International Dimensions
The 505(b)(2) pathway is a U.S.-specific regulatory construct. Other regulatory jurisdictions have their own mechanisms for approving reformulated or modified versions of approved drugs, but they are structured differently and may be more or less permissive depending on the product type.
The European Medicines Agency uses a “hybrid application” process that is conceptually similar to 505(b)(2) — it allows applicants to rely on reference medicinal products for some aspects of their application while conducting new studies for the aspects where the product differs. The EMA’s hybrid pathway is governed by Article 10(3) of Directive 2001/83/EC and has developed its own body of precedent around what data packages are required for different product modifications.
Companies developing 505(b)(2) products for the U.S. market often evaluate whether the same product can be approved in the EU through the hybrid application route, and whether the clinical data generated for the 505(b)(2) application can be used to support the hybrid application with incremental additional data for EU-specific requirements. This global data leveraging is possible in many cases but requires early planning — the clinical study designs for U.S. PK bridging studies and EU equivalent studies are similar but not identical, and a study designed purely for FDA submission may lack specific measurements the EMA requires.
Japan’s Pharmaceuticals and Medical Devices Agency (PMDA) has similar concepts around approval of variations and modified versions of approved drugs, but the Japanese regulatory system has historically been more conservative about reliance on foreign clinical data. Companies bringing 505(b)(2)-style products to Japan typically must conduct Japan-specific bridging studies even when extensive foreign clinical data exists, creating additional data generation requirements.
Part Thirteen: Regulatory Affairs Infrastructure
Building the Right Internal Capability
The regulatory affairs function for a company operating in the 505(b)(2) space requires a specific expertise mix that differs from the expertise needed for NCE development. Understanding FDA’s position on data reliance, having practical experience with bridging study design, knowing how different review divisions interpret the data sufficiency requirements, and understanding the intersection of regulatory strategy with patent strategy are all capabilities that must be present in the regulatory team.
Smaller specialty pharma companies often supplement internal regulatory capacity with external regulatory consultants who have specific 505(b)(2) experience. The best of these consultants bring direct FDA experience — former agency reviewers who understand FDA’s internal deliberative process — combined with practical experience across multiple 505(b)(2) submissions. This combination of inside knowledge and outside perspective is genuinely valuable and commands premium consulting rates.
The risk of relying entirely on external consultants is that institutional knowledge about the company’s product portfolio and competitive strategy doesn’t reside internally. When a key external consultant leaves the engagement, the regulatory strategy work must be reconstructed. Companies that balance external expertise with internal regulatory leadership maintain strategic continuity through personnel changes.
FDA Meetings and Their Strategic Use
The FDA meeting process — Type A, B, and C meetings with different purposes and timelines — is central to effective 505(b)(2) development. Type B meetings include Pre-IND meetings, End-of-Phase 2 meetings, and Pre-NDA meetings, all of which have defined FDA response timelines under PDUFA commitments.
For 505(b)(2) sponsors, the Pre-IND meeting is often the most important meeting in the development program. It is the point at which the FDA can signal whether the sponsor’s proposed approach to data reliance is consistent with what the agency will accept, and what new clinical studies the sponsor will need to conduct to bridge from the reference drug’s data to the new product’s specific characteristics.
Coming into a Pre-IND meeting with a well-prepared briefing document — clearly articulating the proposed product, the reference drug being cited, the nature of the differences, and the proposed data package — maximizes the value of the FDA interaction. Poorly prepared Pre-IND meetings waste both the sponsor’s and the FDA’s time and often produce responses that are too general to guide development planning. The preparation investment in these meetings is one of the highest-return regulatory activities a 505(b)(2) sponsor can make.
The Complete Response Letter and Its Aftermath
A Complete Response Letter (CRL) from the FDA — the agency’s formal notification that an NDA cannot be approved in its current form — is a significant but not unusual event in both 505(b)(1) and 505(b)(2) submissions. The FDA issues CRLs when it identifies deficiencies that must be addressed before approval, ranging from missing data to manufacturing concerns to labeling disagreements.
For 505(b)(2) applications, CRLs frequently cite deficiencies in the bridging data — perhaps the pharmacokinetic bridging study failed to meet the acceptance criteria, or the FDA requires an additional study to characterize the product’s performance in a specific subpopulation. These deficiencies are often addressable with additional studies, but conducting those studies adds six months to two years to the development timeline and meaningful cost to the program.
The strategic imperative is to predict and prevent CRLs rather than respond to them. Pre-NDA meetings provide the opportunity to review draft labeling and identify potential deficiencies before submission. Review of analogous FDA precedents — what data packages the FDA accepted for comparable products — helps predict what the agency will require. Thorough internal review of the application before submission catches gaps that a post-approval Complete Response would otherwise flag.
Conclusion
The Strategic Synthesis
The choice between 505(b)(1) and 505(b)(2) is not a binary decision made once at the beginning of a development program and then forgotten. It is a strategic orientation that shapes every subsequent decision — about target product selection, clinical study design, IP strategy, commercial planning, and capital allocation.
Companies that have internalized the implications of each pathway — and that make development decisions with a clear understanding of which pathway they are pursuing and why — consistently outperform companies that treat the pathway decision as a regulatory technicality.
The 505(b)(1) pathway remains essential for genuinely novel science. When a company has identified a new molecular entity with a mechanism of action that offers substantial therapeutic benefit over existing treatments, the 505(b)(1) pathway is not a choice but a necessity. The higher investment and longer timeline are the cost of doing genuinely new science, and when the science works, the compound patent, NCE exclusivity, and strong secondary IP position can produce commercial returns that justify the investment.
The 505(b)(2) pathway is the appropriate tool when the science of the active ingredient is established and the innovation is in how it is delivered, to whom, or in what combination. Used well, the pathway creates commercially viable pharmaceutical products with attractive economics, faster time to market, and lower clinical risk. Used poorly — by trying to force a product through 505(b)(2) that doesn’t have a genuine reference, or by failing to build adequate IP protection around the 505(b)(2) product — the pathway produces regulatory delays and commercial failures.
The data tools available to pharmaceutical developers today — including the patent expiration tracking and competitive intelligence provided by DrugPatentWatch — allow companies to approach pathway selection with more precision than was possible even a decade ago. The combination of better regulatory precedent, clearer FDA guidance, and more comprehensive competitive data has made 505(b)(2) strategy a discipline rather than an art form. Companies that treat it as a discipline, investing in regulatory expertise, patent intelligence, and commercial due diligence before committing development resources, are the ones consistently generating returns from the pathway.
Key Takeaways
The 505(b)(1) pathway requires all clinical evidence to be generated by or for the applicant — making it the appropriate route for novel molecular entities but carrying development costs that average $2.3 billion and timelines of eight to twelve years.
The 505(b)(2) pathway allows applicants to rely on FDA’s prior findings, published literature, or both — reducing the required clinical investment by 40 to 60 percent compared to conventional NDAs for comparable therapeutic areas, with correspondingly shorter development timelines.
IP protection for 505(b)(2) products requires deliberate construction: the three-year data exclusivity period provided by statute is often insufficient on its own, and sustained commercial exclusivity requires formulation and method-of-use patents layered on top of the regulatory exclusivity.
The Orange Book patent certification process — particularly Paragraph IV certifications — creates predictable litigation risk for 505(b)(2) sponsors, and freedom-to-operate analysis conducted before formulation lock is a mandatory component of competent 505(b)(2) development.
Payer economics matter as much as regulatory strategy: FDA approval of a 505(b)(2) product that cannot command a premium justified by its clinical differentiation produces no commercial return regardless of how elegant the regulatory submission was.
The Inflation Reduction Act’s Medicare drug price negotiation provisions are reshaping the long-term revenue modeling for high-expenditure 505(b)(2) products, particularly those targeting elderly populations with significant Medicare coverage.
Platform-level data tools — including DrugPatentWatch for patent expiration analysis, competitive application tracking, and exclusivity mapping — have made 505(b)(2) competitive intelligence a systematic discipline with measurable impact on development timing and commercial strategy.
Frequently Asked Questions
Q1: Can a company file both a 505(b)(1) NDA and a 505(b)(2) NDA for the same drug in different situations?
A1: Yes, and this happens more often than most people realize. A large pharmaceutical company might file a 505(b)(1) NDA for its novel compound’s primary indication — where it has conducted full Phase III trials and wants NCE exclusivity — while subsequently filing a 505(b)(2) NDA for a new formulation or additional indication of the same compound, relying on its own approved product as the Reference Listed Drug. The 505(b)(2) application in this case references the company’s own prior NDA, which is legally permissible and can accelerate approval of the line extension without requiring the company to repeat work it already submitted. The distinction between the two pathways isn’t tied to the company but to the specific application.
Q2: What happens when the FDA concludes that a proposed 505(b)(2) product actually needs to file as a 505(b)(1) because the available reference data is insufficient?
A2: This is one of the more commercially damaging regulatory redirections a sponsor can experience. If the FDA determines at the Pre-IND meeting — or worse, during NDA review — that the data reliance proposed under 505(b)(2) is inadequate to support approval and that the product effectively requires a full de novo clinical data package, the sponsor faces a fundamental reset of its development program. The entire timeline and budget model must be reconstructed around Phase III trial requirements. The risk of this outcome is highest when the proposed product differs from the reference drug in multiple significant ways simultaneously, when the published literature is thin or of questionable quality, or when the FDA has no prior approval to point to as an adequate safety and efficacy reference. This is why early FDA engagement through a Pre-IND meeting is not optional for 505(b)(2) programs — it is the mechanism by which this catastrophic redirect can be identified and avoided before significant investment is committed.
Q3: How do royalty obligations on background IP affect the economics of 505(b)(2) products built on licensed drug delivery platforms?
A3: Many 505(b)(2) products use proprietary drug delivery technologies that the sponsor licenses from a platform technology company rather than developing internally. The royalty structure on these licenses — typically a percentage of net sales, sometimes with milestone payments — directly affects the commercial economics of the product. A product with a 10% royalty obligation on net sales carries a fundamentally different P&L than the same product without a royalty burden, and sponsors must model these obligations explicitly when evaluating the commercial viability of a 505(b)(2) program. Royalty rates for platform delivery technologies commonly range from 3% to 15% of net sales depending on the technology’s importance to the product’s core value proposition. For a 505(b)(2) product where the delivery system is the central clinical differentiator, royalty rates at the high end of this range can meaningfully compress margins. License negotiation — including most-favored-nation pricing provisions, royalty step-down provisions at defined sales thresholds, and buy-out options — is a commercial skill that competent 505(b)(2) business development functions must bring to every platform licensing negotiation.
Q4: How has the FDA’s application of the “right of reference” concept affected 505(b)(2) development strategy?
A4: The “right of reference” concept is central to understanding what 505(b)(2) sponsors actually get when they cite a Reference Listed Drug. The FDA’s prior review of the RLD’s safety and efficacy is available for the 505(b)(2) applicant to rely upon, but the applicant does not get access to the actual data in the original NDA — that data remains confidential property of the original NDA holder. The FDA acts, in effect, as the bridge: it holds the original data, it has reviewed it and found it adequate, and it will give the 505(b)(2) applicant credit for those findings without disclosing the underlying data. This limitation has practical implications for 505(b)(2) sponsors trying to understand exactly what the FDA found in the original NDA review. The approved labeling, published FDA review summaries, and any publicly available clinical study reports are the primary sources of information about what the original NDA established. Where this information is insufficient to design a bridging study or characterize the reference drug’s PK behavior fully, the 505(b)(2) sponsor must conduct additional characterization studies of the reference drug’s performance — adding to the data package but clarifying the target the 505(b)(2) product must bridge to.
Q5: What lessons does the history of 505(b)(2) abuse-deterrent opioid formulations offer for future reformulation strategies in high-scrutiny therapeutic areas?
A5: The abuse-deterrent opioid 505(b)(2) approvals of the 2010s offer a case study in what happens when a regulatory pathway intersects with a public health crisis. Multiple extended-release opioid formulations with abuse-deterrent properties received 505(b)(2) approvals based on physical or chemical modifications that made products harder to crush, dissolve, or inject. The FDA supported these approvals as harm-reduction strategies while simultaneously trying to limit total opioid prescribing volumes. The commercial and reputational results were mixed. Several products with abuse-deterrent labeling were commercially successful for a period. Others faced payer restrictions that limited their market. All were subject to significant political and public scrutiny about whether the 505(b)(2) pathway was being used to extend market exclusivity on opioids under the cover of a public health rationale. The lesson for sponsors pursuing 505(b)(2) strategies in other high-scrutiny therapeutic areas — including controlled substances, weight-loss drugs, and treatments for behavioral conditions — is that regulatory success does not insulate a product from political or commercial risk. Products approved through technically sound 505(b)(2) applications but perceived as exploiting the pathway for exclusivity rather than patient benefit will face challenges in the payer environment, in congressional scrutiny, and potentially in post-marketing requirements that could not have been predicted at the time of approval. Sponsors in high-scrutiny areas should build the evidentiary case for clinical differentiation — not just regulatory adequacy — before committing to development.
References
[1] Tufts Center for the Study of Drug Development. (2023). Cost to develop and win marketing approval for a new drug. Tufts University.
[2] Food and Drug Administration. (2023). Generic drugs: Questions and answers. U.S. Department of Health and Human Services. https://www.fda.gov/drugs/questions-answers/generic-drugs-questions-answers
[3] Federal Food, Drug, and Cosmetic Act, 21 U.S.C. § 355(b)(2) (1984).
[4] Food and Drug Administration. (1999). Guidance for industry: Applications covered by section 505(b)(2). U.S. Department of Health and Human Services, Center for Drug Evaluation and Research.
[5] Food and Drug Administration. (2020). Guidance for industry: 505(b)(2) applications for drug products containing a previously approved active ingredient. U.S. Department of Health and Human Services, Center for Drug Evaluation and Research.
[6] DiMasi, J. A., Grabowski, H. G., & Hansen, R. W. (2016). Innovation in the pharmaceutical industry: New estimates of R&D costs. Journal of Health Economics, 47, 20–33. https://doi.org/10.1016/j.jhealeco.2016.01.012
[7] Feldman, R. (2018). May your drug price be evergreen. Journal of Law and the Biosciences, 5(3), 590–647. https://doi.org/10.1093/jlb/lsy022
[8] Beall, R. F., Nickerson, J. W., Kaplan, W. A., & Attaran, A. (2016). Is Patent “Evergreening” Restricting Access to Medicine/Device Combination Products? PLOS ONE, 11(2), e0148939. https://doi.org/10.1371/journal.pone.0148939
[9] Wong, C. H., Siah, K. W., & Lo, A. W. (2019). Estimation of clinical trial success rates and related parameters. Biostatistics, 20(2), 273–286. https://doi.org/10.1093/biostatistics/kxx069
[10] Hay, M., Thomas, D. W., Craighead, J. L., Economides, C., & Rosenthal, J. (2014). Clinical development success rates for investigational drugs. Nature Biotechnology, 32(1), 40–51. https://doi.org/10.1038/nbt.2786
[11] Lionberger, R. A. (2008). FDA critical path initiatives: Opportunities for generic drug development. AAPS Journal, 10(1), 103–109. https://doi.org/10.1208/s12248-008-9010-2
[12] Deloitte Centre for Health Solutions. (2022). Measuring the return from pharmaceutical innovation 2022: Balancing risk and reward. Deloitte LLP.
[13] Best Pharmaceuticals for Children Act, Pub. L. No. 107-109, 115 Stat. 1408 (2002); Pediatric Research Equity Act, Pub. L. No. 108-155, 117 Stat. 1936 (2003).
[14] Drug Price Competition and Patent Term Restoration Act of 1984, Pub. L. No. 98-417, 98 Stat. 1585 (1984).
[15] Grabowski, H., Long, G., & Mortimer, R. (2014). Recent trends in brand-name and generic drug competition. Journal of Medical Economics, 17(3), 207–214. https://doi.org/10.3111/13696998.2014.877451
[16] FTC v. Actavis, Inc., 570 U.S. 136 (2013).
[17] Leahy-Smith America Invents Act, Pub. L. No. 112-29, 125 Stat. 284 (2011).
[18] Food and Drug Administration. (2022). Novel drug approvals for 2022. U.S. Department of Health and Human Services. https://www.fda.gov/patients/drug-development-process/novel-drug-approvals-fda
[19] Inflation Reduction Act of 2022, Pub. L. No. 117-169, 136 Stat. 1818 (2022).
[20] Lichtenstein, G. R., Kamm, M. A., Boddu, P., Gubergrits, N., Lyne, A., Butler, T., & Hardi, R. (2007). Effect of once- or twice-daily MMX mesalamine (SPD476) for the induction of remission of mild-to-moderately active ulcerative colitis. Clinical Gastroenterology and Hepatology, 5(1), 95–102. https://doi.org/10.1016/j.cgh.2006.10.025
[21] Food and Drug Administration. (2014). Questions and answers on FDA’s updated CONCERTA (methylphenidate HCl) extended-release tablets labeling. U.S. Department of Health and Human Services. https://www.fda.gov/drugs/drug-safety-and-availability/questions-and-answers-fdas-updated-concerta
[22] Laine, L., Kivitz, A. J., Bello, A. E., Grahn, A. Y., Schiff, M. H., & Taha, A. S. (2012). Double-blind randomized trials of single-tablet ibuprofen/high-dose famotidine vs. ibuprofen alone for reduction of gastric and duodenal ulcers. American Journal of Gastroenterology, 107(3), 379–386. https://doi.org/10.1038/ajg.2011.443
[23] Rosenthal, R. N., Lofwall, M. R., Kim, S., Chen, M., Beebe, K. L., & Vocci, F. J. (2016). Effect of buprenorphine implants on illicit drug use among abstinent adults with opioid dependence treated with sublingual buprenorphine. JAMA, 316(3), 282–290. https://doi.org/10.1001/jama.2016.9quarterly
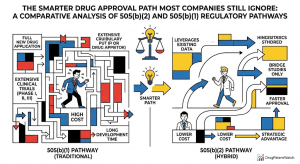
(2) Pathway: Unlocking a Hybrid Strategy for Drug Innovation")
(2) Pathway")
(2) Beats the Branded Generic Every Time — Unless It Doesn't")
(2) Turns Commodities into Cash Cows")

(2): The Smarter Drug Development Path")

(2) Playbook the Big Pharma Textbook Ignores")


(2) Goldmine: How Pharma Extracts Maximum IP Value from Modified Drugs")


(2) Hybrid Patent Strategies for Market Dominance")

(2) and Complex Generic Playbook")
(2) Approval Strategy: The Complete Step-by-Step Guide to a Successful NDA Submission")



(2) Strategy: The Complete Playbook for Portfolio Management, IP Defense, and Generic Launch")
(2) Playbook: Cut Dev Time, Lock In Exclusivity, and Outmaneuver Generics")

(2) Pathway to Build a Differentiated Drug—and Defend It")


