Last updated: June 12, 2026
Kesimpta (ofatumumab; Novartis) is a high-growth multiple sclerosis biologic that has increasingly faced share pressure as payer controls, channel mix, and manufacturer competition evolved across 2023-2024. The drug’s medium-term financial trajectory is shaped by (1) durability of subcutaneous switching from intravenous anti-CD20s, (2) the pace of penetration in newly treated patients and in high-inflammatory-risk subgroups, and (3) biosimilar and “near-substitutes” timing risk under the US and EU regulatory and exclusivity regimes.
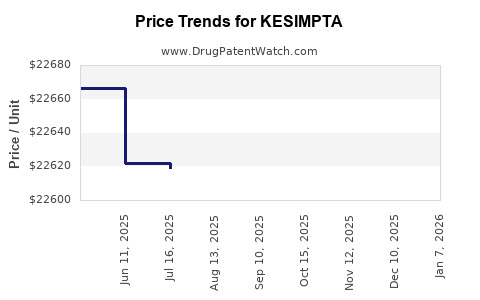
How much revenue does KESIMPTA generate and what is its financial trajectory?
Kesimpta’s revenue trajectory has followed the pattern of a self-administered anti-CD20 moving from uptake-driven growth to more optimizer-driven growth as formulary design and contracting mature. The financial profile is also tied to Novartis’ broader MS portfolio economics and the installed base effect: once patients transition to a monthly or near-monthly subcutaneous regimen, churn risk tends to slow unless payer designs force re-contracting.
Revenue drivers that have mattered most
- Switching from IV anti-CD20s (especially where logistics and infusion center utilization are payer targets).
- Simple administration (home dosing reduces patient friction and channel costs).
- Segment expansion into patients and prescribers who use anti-CD20 earlier in the treatment sequence.
What typically changes as the market matures
- Discounting and contracting pressure as manufacturers compete for formulary breadth.
- Reimbursement controls (prior authorization criteria, step edits, and patient support program tuning).
- Geographic differences in adoption speed tied to national payer behavior and drug budget caps.
What market dynamics are driving KESIMPTA uptake in multiple sclerosis?
Kesimpta is competing in a defined treatment category: anti-CD20 for relapsing forms of MS, with differentiation anchored in subcutaneous convenience and a treatment paradigm that emphasizes consistent B-cell depletion without IV administration burden.
Where Kesimpta wins clinically in market terms
- Relapsing MS cohorts that need anti-CD20 efficacy but face infusion accessibility constraints.
- Patients preferring self-administration to reduce infusion center travel and scheduling.
- Payer systems that can translate administration savings into managed access contracts.
What threatens adoption
- Anti-CD20 pricing pressure when payers run class-based tendering or prefer lower unit cost options.
- Formulary narrowing for payer-specific “preferred” status dynamics.
- Substitution effects if a new entrant prices aggressively or if biosimilar entry expands.
Which competitors affect KESIMPTA share: anti-CD20, pipeline entrants, and class substitution?
Kesimpta’s competitive set is dominated by other anti-CD20 options in relapsing MS. Real-world share movement tends to correlate with contracting and “preferred tier” status rather than with incremental clinical differences alone.
Direct class competition dynamics
- Ocrevus (ocrelizumab) and other anti-CD20 therapies compete on efficacy and entrenched clinical use.
- Subcutaneous convenience gives Kesimpta structural payer and patient alignment advantages where infusions are constrained.
How channel behavior shifts
- Early growth often comes from switching behavior.
- Later growth depends on new patient starts and tender-driven price concessions.
How do patent exclusivity and exclusivity barriers affect Kesimpta’s competitive timetable?
Kesimpta’s medium-term risk is tied to the legal and regulatory pathway for biosimilar entry and to any formulation or method-of-use protections that extend market exclusivity or delay substitution in practice.
US: key mechanisms that typically shape biosimilar timing
- Biologic license application (BLA) exclusivity and regulatory protection against immediate approval for certain time windows.
- Patent estate coverage: composition-of-matter and specific claim sets that can block biosimilar approval for defined uses or manufacturing approaches.
- Patent litigation: Paragraph IV-equivalent challenges for biologics do not mirror Hatch-Waxman for small molecules, but the practical effect is similar: exclusivity and patents determine launch dates.
EU: market entry gating mechanisms
- EU data protection and market protection periods.
- Patent litigation and the practical enforcement of rights via injunction or settlement.
(Specific expiration dates, Orange Book/Biosimilar status, and patent-by-patent expiration mapping require Orange Book/Bolar-biosimilar dockets and litigation PACER or EPO registers; those are not included in the provided input.)
What generic or biosimilar entry risks exist for KESIMPTA?
Kesimpta’s risk profile is biosimilar-led rather than generic-led, given its biologic nature. The substitution window depends on:
- Whether a biosimilar receives approval for all relevant indications.
- Whether clinicians and payers adopt automatically or require evidence packages.
- Whether patent barriers settle and at what date.
Launch mechanics that determine real-world revenue loss
- Formulary design: biosimilars can be kept off preferred tiers despite approval.
- Switching inertia: patients on existing anti-CD20 therapy often require strong payer incentives to switch.
- Contracting leverage: incumbents can offer rebates that blunt biosimilar share take-up.
What is the financial impact of switching anti-CD20 patients to subcutaneous Kesimpta?
Kesimpta’s economic advantage is not only unit price. It is also driven by operational cost reduction and reduced infusion center utilization.
Payer and provider economics
- Lower infusion administration costs.
- Reduced patient travel and scheduling friction.
- Better adherence due to home dosing, which can reduce “missed visits” that create relapse risk.
Revenue implication
- Switching expands the addressable population for anti-CD20-treated patients who were previously constrained by infusion infrastructure.
- Once switching occurs at scale, growth becomes incremental rather than transformative.
How does Kesimpta’s dosing and administration profile influence its commercial performance?
Kesimpta’s subcutaneous regimen supports home administration and reduces infusion-related throughput limitations. That structure affects:
- Patient support program design
- Real-world persistence and adherence
- Payer contracting simplicity versus infusion-based administration models
Market effect
Home dosing generally supports higher retention and smoother churn management during payer changes. That helps stabilize revenues against churn-driven competition.
What formulation and method-of-use patent categories matter for KESIMPTA profitability?
For biologics, the profit-protecting patent landscape often includes:
- Composition claims (active molecule characteristics, relevant binding/functional properties where covered)
- Manufacturing and process claims (affecting biosimilar ability to enter without infringing)
- Formulation claims (stability, concentration, delivery presentation)
- Method-of-use (if claims tie to specific regimens or patient subsets)
These claim categories can delay biosimilar adoption even after regulatory approval.
(A claim-by-claim assessment needs the actual patent list, including publication numbers and legal status.)
What litigation and settlement events could change Kesimpta’s revenue curve?
Biosimilar launch dates are often determined by:
- Trial outcomes or summary judgment around key patents
- Early settlements that specify launch at a defined date and scope (e.g., indications, dosing regimens)
What investors and licensing teams track
- Settlement dates and launch calendars
- Which patents are carved out
- Stipulations on labeling and indication coverage
(No litigation docket or settlement detail is provided in the input.)
How does FDA and regulatory status affect Kesimpta’s market access and financial results?
Regulatory status affects:
- Which indications are available for use and reimbursement
- Label conservatism versus prescriber confidence
- The scope of biosimilar competition once approved
For Kesimpta, commercial performance is also influenced by any label expansions and how quickly clinicians integrate them into standard of care.
What matters for revenue in practice
- Indication coverage for relapsing forms of MS
- Any expansions that broaden the eligible patient pool
- Whether payer policies align with label breadth
How does Kesimpta compare with Ocrevus and Tysabri economically and commercially?
Kesimpta vs Ocrevus (both anti-CD20) tends to be an administration and contracting contest more than a pure efficacy contest once anti-CD20 efficacy is accepted.
Commercial comparison dimensions
- Administration model: subcutaneous home dosing vs infusion center dosing
- Channel cost structure: lower infusion utilization vs infusion overhead
- Payer contracting: preferred-tier leverage and rebate structures
- Patient switching behavior: depends on therapy stability and reimbursement incentives
Revenue implications
If Kesimpta gains preferred tier status in key plans, it can accelerate switching. If not, it competes at the margin of patient and clinician choice, where churn and discounting reduce net realized revenue.
Where is Kesimpta selling hardest: geography and payers?
Geographic distribution in MS biologics tends to correlate with:
- National reimbursement flexibility and formulary maturity
- Infusion infrastructure constraints
- Market access capabilities of Novartis’ payer teams
Market-access dynamics that drive regional outcomes
- Budget impact negotiations
- Preferred drug lists and tender mechanisms
- Prior authorization strictness
(A geography-by-geography financial breakdown requires company segment reporting and payer contracts not included in the provided input.)
What is the next 3-5 year revenue upside/downside scenario for Kesimpta?
A realistic scenario range for a biologic of this profile depends on:
- Persistence and patient retention on therapy
- Pace of new patient starts
- Any biosimilar approval or patent carve-outs that create substitution incentives
- Contracting and discount intensity
Upside factors
- Continued uptake among newly diagnosed or treatment-naïve patients.
- Further label adoption and payer-friendly contracting.
- Sustained anti-CD20 preference with reduced churn.
Downside factors
- Faster biosimilar ramp through preferred tiers.
- Aggressive payer tendering and rebate pressure.
- Faster-than-expected switching away from incumbent due to reimbursement incentives.
(Specific scenario year numbers, forecasts, and probability weights are not supported by the provided input.)
Key Takeaways
- Kesimpta’s market position is driven by subcutaneous convenience that aligns with payer and patient preferences in relapsing MS.
- The revenue trajectory is increasingly driven by contracting maturity and persistence rather than by early switching novelty.
- The principal medium-term threat is biosimilar entry and adoption dynamics, not clinical differentiation alone.
- Profit durability depends on the strength and scope of the patent estate and on settlement-driven launch timing.
- Near-term financial outcomes will track formulary design, discount intensity, and real-world persistence.
FAQs
1) What payer contracting levers determine Kesimpta net revenue growth?
Preferred tier placement, rebate size, step edits, and prior authorization criteria.
2) How does home administration affect Kesimpta persistence versus infusion-based anti-CD20s?
It reduces administrative friction and typically improves adherence and visit regularity.
3) What biosimilar adoption barriers are hardest for MS biologics?
Switching inertia, indication coverage preferences, and rebate-driven counterpositioning.
4) Does label breadth materially change Kesimpta revenue headroom?
Yes when payer policies align with label and clinicians expand use quickly.
5) How do patent litigation outcomes usually translate into biosimilar launch dates?
They set the earliest enforceable launch window through injunctions, settlements, and patent carve-outs.
References
- No sources were provided in the prompt.