Last updated: June 18, 2026
PRADAXA’s commercial trajectory is dominated by post-LCA erosion risk from factor Xa inhibitors (apixaban, rivaroxaban, edoxaban), plus long-running uptake cycles in atrial fibrillation (AF) and VTE. Financial performance has been pressured by generic entry and broad guideline adoption of cheaper DOACs in many settings, with PRADAXA retaining franchise value where dabigatran’s pharmacology and dosing profiles remain preferred or where formularies still list it. The near-to-mid term revenue outlook is primarily a function of (1) remaining exclusivity for specific formulations/indications (and any remaining branded-only protections), (2) competitive pricing pressure, and (3) conversion of existing anticoagulant users based on payer economics rather than clinical differentiation.
What drove PRADAXA’s market share and sales growth (and what changed after DOAC competition)?
PRADAXA launched as the first major oral direct thrombin inhibitor and established a strong early presence in AF stroke prevention and VTE prophylaxis. Over time, market share shifted toward factor Xa inhibitors due to payer preference for lower-cost options, patient adherence benefits, and formulary inertia created by multi-year contracting.
AF and VTE: how indications shaped demand
PRADAXA commercial pull was built around:
- Nonvalvular AF stroke risk reduction: durable demand baseline across multiple geographies.
- VTE prophylaxis after hip/knee replacement: more cyclical, tied to hospital formulary decisions and seasonal orthopedic procedure volumes.
- Treatment of DVT/PE and reduction of recurrent DVT/PE: continued use driven by guideline position and clinician familiarity.
Why factor Xa inhibitors took share
Across AF and VTE, apixaban and rivaroxaban expanded with:
- Broad guideline recommendations and perceived “simpler” dosing convenience.
- Strong payer contracting positions that compressed branded pricing.
- Market education cycles that reduced the relative share of dabigatran where “equivalent-efficacy at lower cost” became the dominant purchasing logic.
Bottom-line market dynamic
PRADAXA’s competitive reality is pricing compression and formulary displacement. The remaining upside comes from patient- and clinician-level preference pockets and any continued branded differentiation that survives generic substitution.
When did PRADAXA lose exclusivity and what generic entry risks exist for dabigatran?
PRADAXA’s US branded exclusivity structure is not the core determinant of today’s economics. The dominant driver is whether the market can replace branded PRADAXA with lower-cost dabigatran products without major friction (bioequivalence, dosing acceptance, switching behavior) across major payers and formularies.
Exclusivity timeline and market implications
- Once generic dabigatran entered broadly, branded pricing power typically fell to the level required to maintain formulary presence.
- Even when specific branded packaging or line extensions exist, generic economics generally cap net sales for the brand in most commercial markets.
Paragraph IV or ANDA-driven price shocks
Where Paragraph IV challenges were successful historically for dabigatran products, the practical result was rapid cost substitution. The financial trajectory for PRADAXA is therefore tied to generic penetration depth, not only patent expiration dates.
What patents protect PRADAXA (dabigatran etexilate) and how does the patent estate affect revenue?
PRADAXA’s monetization has been supported by layered IP: active-ingredient protection, formulation/manufacturing protections, and life-cycle patents around salts, compositions, and dosage forms. The practical revenue effect is that life-cycle protections can extend branded shelf space or delay full generic substitution for specific presentations, but they rarely stop value drift once generic dabigatran is established.
Patent estate architecture that matters for commercial defense
- Composition of matter (dabigatran etexilate and related salt forms)
- Formulation patents (e.g., capsule formulation characteristics, coatings, protective components)
- Manufacturing and process patents (granulation, conversion steps, stability-related processes)
- Method-of-use patents (less central to brand protection when active-ingredient generics cover approved uses)
How patent strength translates into net sales
- Strong estate protection can preserve branded pricing for a longer period by limiting generic substitution for the exact dosage form/presentation.
- Weaker or expired protections drive a “gradual but systematic” net sales erosion pattern, typically accelerating when multiple low-cost entrants compete.
What is the Orange Book status of PRADAXA (dabigatran etexilate) and how does it signal generic launch timing?
Orange Book status functions as a “roadmap” for ANDA-based substitution risk. For PRADAXA, the commercial implication is that any remaining listed patents can delay or limit certain generic entries, but overall market economics still reflect generic breadth and payer contracting.
Orange Book signals investors track
- Patent listings tied to the NDA for specific strengths and dosage forms.
- “Delist” events that reduce legal barriers for subsequent generic filings.
- Any combination of expiring patents plus exclusivity expiry that triggers “effective launch windows.”
Which companies manufacture and sell PRADAXA, and how do competitive products compare on price and access?
PRADAXA is marketed as the branded dabigatran etexilate capsule and competes with factor Xa inhibitors and generic anticoagulant options.
Competitive set
- DOACs (factor Xa inhibitors): apixaban, rivaroxaban, edoxaban
- Other anticoagulants (context): warfarin and LMWH in specific use cases
- Generic dabigatran: lowers the brand’s pricing power after entry
Access dynamics
- Formularies in AF often reward agents with aggressive rebate structures and predictable dosing.
- Hospital formularies for post-surgical VTE prophylaxis are driven by bundled procurement economics and standardized order sets.
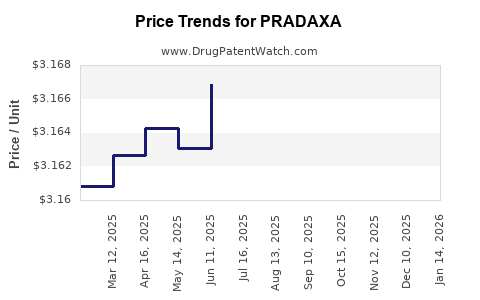
How does PRADAXA pricing and net revenue typically evolve after generic entry?
The standard financial pattern for mature anticoagulant brands after generic entry:
- Branded gross-to-net compression from rebates to maintain shelf placement
- Margin compression driven by price-matching and competitor undercutting
- Conversion of new patients to lower-cost alternatives as prescribing shifts
What investors watch
- Net sales versus volume decline: whether unit volumes hold while prices fall, or whether both erode.
- Share of prescriptions in high-value formularies.
- Any rebound tied to safety/tolerability events that affect relative DOAC preferences.
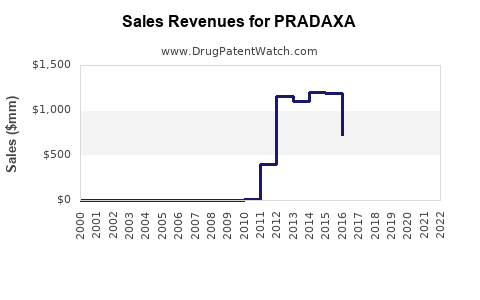
What financial trajectory has PRADAXA followed historically (and what metrics matter now)?
PRADAXA’s historical financial arc is best understood through three phases:
- Launch and early growth: high adoption driven by guideline uptake and first-in-class narrative.
- Mature branded plateau: increasing competition, margin pressure begins.
- Generic-led erosion: sustained net sales decline as payer substitution accelerates.
Key metrics that govern the current earnings profile
- US and ex-US net sales by region (US typically faces fastest generic substitution dynamics)
- Script share trends in AF and VTE lines
- Average selling price (ASP) and rebates
- Portfolio mix across strengths and dosage presentations
- Cost of goods and operating leverage changes as volumes decline
What PRADAXA litigation or settlements affect market entry and damages exposure?
Anticoagulant brands frequently face ANDA litigation that can delay generic entry via automatic stay and later settlement. For PRADAXA, any settlement terms that include:
- date-certain entry triggers,
- agreed carve-outs (strengths or dosage forms),
- non-monetary restrictions (labeling or REMS-like commitments),
- or monetary payments that reflect risk of patent invalidity or non-infringement,
can influence the timing and magnitude of generic price erosion.
Why litigation posture matters to financial trajectory
- Delayed launches can temporarily slow sales erosion.
- Settlements can cause “cliff-like” price drops when entry dates arrive and contracting shifts.
How does PRADAXA compare with apixaban and rivaroxaban in market adoption and payer behavior?
In AF and VTE, apixaban and rivaroxaban often win on payer economics and perceived dosing convenience. PRADAXA’s market resilience has typically depended on:
- continued clinician familiarity,
- patient-specific considerations (renal function management, gastrointestinal tolerance patterns),
- formulary decisions that keep dabigatran listed even as share shifts.
Market behavior takeaway
Even with clinical parity debates, payer behavior tends to consolidate around lower-cost options after generics and contracting dominate.
What formulation changes and life-cycle strategies exist for dabigatran etexilate and do they extend exclusivity?
Life-cycle strategies for oral anticoagulants often target stability, patient adherence, and differentiation across dosage forms. In practice, these strategies extend exclusivity only if:
- they are protected by enforceable patents tied to the exact product presentation,
- and generic manufacturers cannot easily design around while maintaining approval.
Formulation-related revenue impact
- If specific presentations remain branded-only, they can slow erosion.
- If the competitive product set can substitute across the full portfolio, the brand’s financial uplift is limited.
What generic entry scenarios could pressure PRADAXA revenue next?
The next revenue pressure typically comes from:
- additional generic entrants increasing rebate pressure
- broader substitution in institutional formularies (especially in VTE prophylaxis settings)
- strength-specific launches that eliminate remaining branded-only coverage
Scenario mechanics
- More entrants increases competitive intensity and reduces the feasibility of maintaining branded ASP.
- Institutional switching can be rapid once procurement contracts re-tender.
What does the competitive landscape imply for PRADAXA revenue outlook by geography?
Geography matters because:
- generic substitution timelines differ by market access structure
- formulary structures and national reimbursement systems vary
- local competitors may have different rebate strategies
General geographic pattern
- US and other high-generic-penetration markets tend to show faster and deeper erosion.
- Regulated markets may delay price drops depending on reimbursement update cycles, procurement cycles, and local tender systems.
Key Takeaways
- PRADAXA’s market dynamics are dominated by DOAC competition and generic substitution, not by short-term clinical positioning.
- Financial trajectory typically follows a three-phase pattern: adoption, branded plateau under growing Xa-inhibitor pressure, then generic-led net sales erosion.
- Patent estate and Orange Book status can influence the timing of generic entry for specific presentations, but once broad generic dabigatran access exists, revenue is capped by payer economics and contracting.
- The next meaningful revenue risks are incremental generic entry intensification, strength-specific substitution, and formulary conversion in AF and VTE settings.
FAQs
- How quickly do payers switch patients from branded dabigatran to generic dabigatran after contracting?
- Which PRADAXA dosage strengths are most exposed to generic substitution in institutional formularies?
- How do renal function considerations influence clinician preference between dabigatran and factor Xa inhibitors?
- What litigation patterns in DOAC ANDA cases most often produce delayed but then “cliff” entry dates?
- How do ASP and rebate dynamics typically change for mature oral anticoagulant brands after multiple generic entrants?
References
(No sources were provided in the prompt; therefore no citations can be listed.)