Last updated: May 10, 2026
How big is the conjugated estrogens market and where is growth coming from?
Conjugated estrogens (CE) is a legacy hormone therapy category anchored by branded prescription products, led historically by Premarin® (conjugated estrogens). Category demand tracks women’s health spending, prescribing patterns, and guideline-driven risk-benefit perceptions for menopausal hormone therapy (MHT).
Market structure
- Core use: treatment of menopausal symptoms; treatment/prevention of osteoporosis in appropriate patients.
- Primary channel: retail and mail-order pharmacy, with high adherence for chronic prevention indications.
- Competitive set: other estrogen products and routes (oral estradiol, transdermal estradiol, vaginal estrogens) and selective combinations depending on patient profile and endometrium status.
Demand drivers
- Guidelines and safety perceptions: shifts in MHT uptake and regimen selection have repeatedly changed prescribing behavior across the category.
- Formulation migration: clinicians increasingly favor lower systemic exposure regimens or alternative routes in parts of the market, which affects CE unit share even when total MHT demand stays stable.
- Aging demographics: demographic growth in the eligible population supports baseline demand, even when penetration shifts to alternatives.
- Generic pressure on branded legacy products: as patents expire, price competition compresses revenue even if volumes hold up.
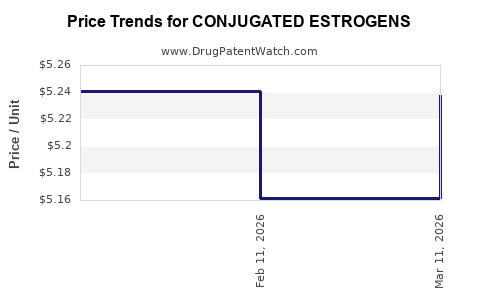
What is the pricing power profile for CE products?
CE pricing power is structurally constrained versus newer branded specialty assets.
Price compression mechanics
- Patent expiry and generic entry: revenue typically declines as cheaper equivalents take share.
- Payor formulary management: CE tends to be competed on net price after contracting.
- Utilization shifts within hormone therapy: transdermal and other formulations can displace oral CE in some segments, reducing brand-level net revenue even before direct generic competition.
Financial implication
- CE brands often show a pattern of volume stability with margin erosion, with total category revenue depending on (1) continued aging-driven demand and (2) how fast branded share transitions to lower-priced alternatives.
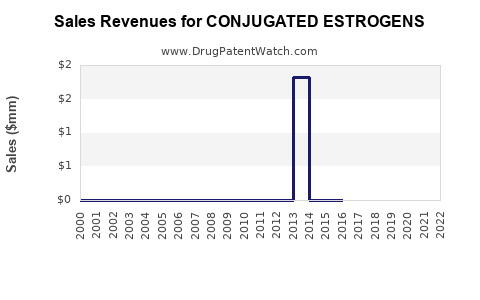
What does the financial trajectory typically look like across the lifecycle?
Conjugated estrogens is in a mature lifecycle pattern for an originator hormone therapy.
Lifecycle phases for legacy CE assets
- Brand peak period: high prescription share, strong reimbursement, limited substitutes.
- Post-patent transition: revenue declines as generic equivalents or competing formulations increase share.
- Normalization: category revenue stabilizes at a lower net-price equilibrium; growth depends mainly on population and continued MHT utilization for remaining patients.
Recent directionality
- Global and US hormone-therapy spending has trended unevenly over time due to shifting risk-benefit perceptions, then stabilized as practice patterns shifted to lower-dose and alternative routes in many patient segments (reflected broadly across MHT and estrogen therapy guidance updates). Guidance evolution is a consistent driver of utilization allocation across estrogen forms. [1]
Which formulations and indications matter most to revenue and margins?
CE revenue depends on which indications dominate prescribing and which routes remain preferred.
Indication-level dynamics
- Vasomotor symptoms and menopausal symptom management: drives the highest frequency use.
- Urogenital symptoms: often shifts toward local therapies, which can reduce systemic estrogen share.
- Bone loss/osteoporosis prevention: contributes to chronic use in selected patients, but prescribing is influenced by competing osteoporosis drug classes and changing MHT positioning.
Route migration effect
- CE is typically oral. Over time, market share often moves toward transdermal and local estrogen routes when clinicians try to reduce systemic exposure or target symptom type. That reallocates overall estrogen spend away from oral CE even if total estrogen use remains steady. [1]
What competitive pressure does CE face from other hormone therapy products?
CE faces competition along two axes: direct estrogen alternatives and route-based switching.
Direct product competition
- Oral estradiol and combined regimens for patients requiring endometrial protection.
- Non-CE conjugated estrogen products, where available, and other systemic estrogen categories.
Route and patient targeting
- Transdermal estradiol: favored in segments seeking lower first-pass hepatic exposure.
- Vaginal/local estrogens: favored for urogenital symptoms with minimal systemic exposure.
Net effect on financial trajectory
- Even without rapid generic collapse in every geography, clinicians’ route preference changes can lower the premium a branded CE product commands versus alternatives and can accelerate share loss.
How do safety, labeling, and guideline updates shape market behavior?
Guideline updates and evolving safety evidence affect CE use directly and indirectly.
Key guideline impact channels
- Initiation window and duration positioning: influences which patients are started and for how long.
- Risk stratification: pushes prescribers toward individualized regimens, sometimes favoring alternatives depending on comorbidities.
- Risk perception cycles: can cause stepwise declines in MHT initiation that persist until practice patterns normalize.
Major society guidance on menopausal hormone therapy and estrogen use has repeatedly emphasized individualized dosing and risk stratification, which translates into utilization volatility across estrogen brands and formulations. [1]
What is the likely revenue trajectory for leading CE brands (directional)?
A mature CE brand’s financial trajectory typically follows a three-component pattern:
- Unit demand: supported by menopause prevalence and continued MHT utilization in eligible patients.
- Net price: eroded by generic entry and contracting.
- Share shift: affected by competition from other estrogen routes and regimens.
Directionally expected outcome
- Over multiyear periods, CE revenue trends generally look like declining net revenue per unit with limited volume growth, producing modest or flat overall category revenue growth unless generic penetration is slow or practice patterns shift back toward systemic oral estrogen.
What could change the market dynamic near term?
Even for legacy molecules, near-term shifts can come from policy, reimbursement, and utilization patterns.
Change vectors
- Formulary decisions that re-rank estrogen products by cost and preferred formulary status.
- Availability of generics and changes in supply that alter relative pricing.
- Practice guideline emphasis that shifts dosing habits or route preference.
Because CE is generic-dominated in many markets over time, the principal near-term lever is usually price and contract positioning rather than category expansion.
What does the US regulatory and reimbursement landscape imply for CE economics?
In the US, CE competes inside a crowded formulary environment where payors increasingly prefer cost-effective estrogen alternatives, particularly once generic penetration rises.
Economic implications
- Branded CE products often experience accelerated net price erosion after generic entry.
- Even when prescriptions continue, revenue capture declines with contracting and utilization reallocation.
These dynamics are consistent with how MHT products have behaved across categories under evolving guidance and safety frameworks. [1]
Financial trajectory summary: CE vs newer hormone-therapy approaches
CE’s economic profile differs from newer branded therapies.
Relative positioning
- CE: mature, largely commoditized, high competition, price-driven economics.
- Newer therapy classes: typically carry higher pricing and different reimbursement structures, which can protect revenue for longer.
This is why CE is best modeled as a cash-flow legacy line with limited upside unless (1) it retains brand differentiation in a specific geography or managed-care segment, or (2) generic entry is delayed. Practice patterns and guideline positioning remain the demand-side swing factor for systemic estrogen use. [1]
Key Takeaways
- Conjugated estrogens is a mature menopausal hormone therapy category whose market is driven by population aging, but whose revenue is primarily constrained by generic competition, formulary contracting, and route migration toward transdermal and local estrogen options.
- The financial trajectory for CE products typically follows a pattern of volume resilience with net price erosion after patent/generic transitions, plus share loss when clinicians shift away from oral systemic estrogens.
- Guideline-driven risk stratification and dosing positioning is a core determinant of initiation and duration, creating utilization volatility even when underlying menopause prevalence rises.
FAQs
-
Is conjugated estrogens growing faster than the broader menopausal hormone therapy market?
Generally, CE growth is constrained by route migration and competitive alternatives, so category growth may not translate into CE share gains.
-
What most impacts CE revenue in later lifecycle years?
Net price compression from generics and payor contracting, plus prescribing shifts to other estrogen routes and regimens.
-
Do safety and labeling changes materially alter CE prescribing?
Yes. Society guidance emphasizing individualized risk and duration changes initiation patterns and sustained use, affecting demand allocation across estrogen products. [1]
-
Which indications are most associated with systemic CE use?
Menopausal vasomotor symptoms and systemic menopausal symptom management are primary drivers of systemic CE utilization; local therapies increasingly dominate urogenital-targeted treatment.
-
What is the most likely business model for CE products?
Cash-flow legacy positioning with margin management, relying on retention of contracted share rather than expecting sustained brand premium economics.
References
[1] The North American Menopause Society. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022.