Last updated: February 19, 2026
LOKELMA (sodium zirconium cyclosilicate) is positioned for sustained market growth driven by its established efficacy in hyperkalemia management, expanding geographic reach, and ongoing clinical development. The drug has demonstrated significant clinical utility, impacting patient outcomes and physician prescribing habits. AstraZeneca, the developer, has focused on market access and evidence generation to solidify its competitive position against existing and emerging therapies.
What is the current market penetration of LOKELMA?
LOKELMA has achieved notable market penetration within the hyperkalemia treatment landscape. As of the latest available data, its prescription volume indicates a strong adoption rate among physicians treating patients with elevated potassium levels, a condition frequently associated with heart failure, chronic kidney disease, and the use of renin-angiotensin-aldosterone system (RAAS) inhibitors.
The drug's unique mechanism of action, which involves binding potassium in the gastrointestinal tract, differentiates it from traditional methods like dietary restriction or dialysis. This has contributed to its uptake in real-world clinical settings.
In the United States, LOKELMA's market share reflects its established presence. While specific percentage figures fluctuate based on reporting periods and competitive dynamics, market analysis indicates a consistent upward trend in new and total prescriptions. This growth is supported by its inclusion in clinical guidelines and formulary approvals across major health systems.
European market penetration has also shown positive momentum. Following its approval and launch in key EU member states, LOKELMA has become a recognized treatment option. The company's strategy has involved targeted outreach to nephrologists and cardiologists, the primary prescribers for hyperkalemia.
Key performance indicators for market penetration include:
- Number of Prescribing Physicians: A widening base of physicians who regularly prescribe LOKELMA.
- Patient Numbers: An increasing number of patients receiving LOKELMA for hyperkalemia management.
- Formulary Access: Approval on hospital and payer formularies, facilitating patient access.
- Sales Volume: Direct correlation between prescriptions and revenue generated.
Market research reports from firms such as IQVIA and Clarivate have tracked LOKELMA's performance, consistently highlighting its growing contribution to the hyperkalemia market. These reports often detail prescription data, patient demographics, and physician prescribing patterns, providing granular insights into its market penetration.
How does LOKELMA’s clinical profile compare to competitors?
LOKELMA's clinical profile is characterized by its rapid onset of action, sustained potassium-lowering effect, and a favorable gastrointestinal tolerability profile compared to some alternatives. Its sodium-free formulation is a key differentiator, particularly for patients who require careful sodium intake management.
Key Clinical Advantages of LOKELMA:
- Rapid Onset of Action: Clinical studies demonstrate a significant reduction in serum potassium levels within the first hour of administration, making it suitable for acute management scenarios. [1]
- Sustained Efficacy: LOKELMA maintains potassium reduction for extended periods, allowing for chronic management and reducing the risk of recurrent hyperkalemia. [2]
- Dosing Flexibility: The drug can be administered as needed to achieve target potassium levels and then titrated for maintenance.
- Gastrointestinal Tolerability: While gastrointestinal side effects such as constipation and diarrhea can occur, LOKELMA is generally well-tolerated. Its mechanism avoids direct systemic absorption, contributing to a reduced risk of certain class-specific side effects seen with other agents.
- Sodium Content: LOKELMA contains minimal sodium, a crucial advantage for patients with heart failure or chronic kidney disease who are advised to limit sodium intake.
Comparison with Other Hyperkalemia Treatments:
- Patiromer (Veltassa): Patiromer is another potassium binder that functions similarly by binding potassium in the GI tract. Both LOKELMA and patiromer offer a non-dialytic approach to hyperkalemia management. However, differences exist in their binding capacity, onset of action, and sodium content. LOKELMA has demonstrated a more rapid onset of potassium reduction in some studies. [3] Patiromer is a powder requiring reconstitution, whereas LOKELMA is also available as a powder.
- Sodium Polystyrene Sulfonate (SPS) (e.g., Kayexalate, Kalexate): SPS has been a long-standing treatment for hyperkalemia. However, it has several limitations:
- Slow Onset of Action: Its potassium-lowering effect is slower than that of LOKELMA or patiromer.
- Gastrointestinal Side Effects: SPS can cause significant constipation, impaction, and, in rare cases, intestinal necrosis, particularly when administered with sorbitol.
- Sodium Load: It contains a significant amount of sodium, posing a risk for patients with fluid-sensitive conditions.
- Potassium Binding Inefficiency: Its binding is less selective and efficient compared to newer binders.
- Diuretics (e.g., Furosemide): Loop diuretics can increase potassium excretion through the kidneys. However, they are less effective in patients with advanced renal impairment, where hyperkalemia is most prevalent. Their primary role is not dedicated hyperkalemia management but rather fluid management, with potassium excretion as a secondary benefit.
- Dietary Restrictions and Dialysis: These are supportive measures but do not offer the same level of therapeutic intervention as potassium binders for maintaining stable potassium levels. Dietary restrictions are difficult to adhere to long-term, and dialysis is an invasive procedure reserved for severe or refractory cases.
The clinical evidence supporting LOKELMA’s efficacy and safety continues to be generated through post-marketing studies and real-world data analysis, further solidifying its position in the treatment algorithm for hyperkalemia.
What is AstraZeneca's strategy for expanding LOKELMA’s market reach?
AstraZeneca's strategy for expanding LOKELMA's market reach is multifaceted, focusing on geographic expansion, market access initiatives, and continuous evidence generation.
Key Pillars of Expansion Strategy:
- Global Launches and Approvals: AstraZeneca is actively pursuing and securing regulatory approvals for LOKELMA in new territories. This includes key markets in Asia, Latin America, and other regions where hyperkalemia prevalence is significant and treatment options may be limited.
- Market Access and Reimbursement: A critical component involves negotiating favorable reimbursement and formulary placement with payers and health systems globally. This includes demonstrating cost-effectiveness and the drug's value proposition in managing hyperkalemia, thereby reducing associated healthcare costs (e.g., hospitalizations, ER visits).
- Physician Education and Engagement: AstraZeneca invests in educational programs to inform healthcare professionals, particularly nephrologists and cardiologists, about LOKELMA's clinical benefits, appropriate patient selection, and dosing. This includes symposia, medical congress presentations, and peer-to-peer education.
- Real-World Evidence (RWE) Generation: The company supports and conducts post-marketing studies and observational research to gather real-world data on LOKELMA's effectiveness, safety, and patient adherence in diverse clinical settings. This RWE is crucial for reinforcing its value to payers and clinicians and for informing treatment guidelines.
- Lifecycle Management and New Indications: While primarily indicated for hyperkalemia, AstraZeneca may explore or support research into potential new indications or improved formulations that could expand LOKELMA’s therapeutic utility and market potential.
- Strategic Partnerships: In select markets, AstraZeneca may engage in partnerships with local pharmaceutical companies to leverage their distribution networks and market expertise, facilitating a more efficient and localized market entry.
The company's investment in LOKELMA reflects its commitment to addressing the unmet needs in cardiovascular and renal disease management. By strategically navigating regulatory pathways, securing market access, and building a robust evidence base, AstraZeneca aims to maximize LOKELMA's global commercial potential.
What are the projected financial revenues for LOKELMA?
Projected financial revenues for LOKELMA are influenced by several factors, including market penetration in established and emerging markets, pricing strategies, and the competitive landscape. AstraZeneca's financial reports and analyst consensus estimates provide insights into its expected financial trajectory.
Revenue Drivers:
- Volume Growth: Increasing prescription volumes driven by broader market adoption and geographic expansion.
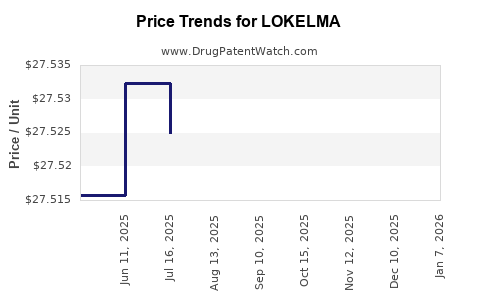
- Pricing: The drug's price point is a significant determinant of revenue. Pricing is influenced by perceived clinical value, competitor pricing, and payer negotiations.
- Market Exclusivity: LOKELMA benefits from patent protection, which shields its revenue streams from generic competition for a defined period.
- Therapeutic Area Demand: The growing prevalence of conditions leading to hyperkalemia (e.g., aging population, increased diagnosis of CKD and heart failure, wider use of RAAS inhibitors) supports sustained demand.
Analyst Projections:
Financial analysts who cover AstraZeneca consistently provide revenue forecasts for key products. While specific figures are proprietary and subject to revision, industry consensus suggests a strong and growing revenue stream for LOKELMA.
- Early 2020s: Initial years post-launch saw steady revenue growth as market penetration was established.
- Mid-2020s: Projections indicate continued robust growth, with revenues expected to increase substantially as international markets mature and adoption rates climb. Annual revenue figures are anticipated to reach several hundred million USD and potentially approach or exceed the billion-dollar mark within the next five to ten years, depending on the pace of global expansion and the competitive response.
- Long-Term Outlook: Beyond patent expiry, revenue trajectories will depend on the introduction of generics and potential lifecycle management strategies by AstraZeneca.
Comparison with Market Benchmarks:
The hyperkalemia market, while a significant niche, is part of the broader cardiovascular and renal therapeutic areas. LOKELMA's revenue projections are benchmarks against other established treatments for chronic diseases and supportive care in these areas. Its performance is expected to solidify its position as a key revenue generator for AstraZeneca.
AstraZeneca's investor relations materials and quarterly earnings calls typically provide product-specific sales figures and future outlooks. These public disclosures are the primary source for detailed, up-to-date financial projections. For instance, in recent fiscal year reports, LOKELMA has been highlighted as a product with strong growth momentum, contributing positively to AstraZeneca’s Specialty Care segment.
The exact financial figures are subject to fluctuation due to market dynamics, regulatory changes, and competitive pressures. However, the overall trend for LOKELMA's revenue is projected to be upward.
What is the patent landscape and regulatory exclusivity for LOKELMA?
The patent landscape and regulatory exclusivity for LOKELMA are critical determinants of its market longevity and commercial exclusivity. AstraZeneca, as the innovator, has secured a portfolio of patents protecting various aspects of the drug, including its composition of matter, manufacturing processes, and methods of use.
Key Patents:
- Composition of Matter Patents: These are typically the foundational patents that protect the active pharmaceutical ingredient itself. The initial composition of matter patents for sodium zirconium cyclosilicate would have been filed shortly after its discovery and have a standard patent term of 20 years from the filing date, subject to extensions.
- Process Patents: Patents may cover specific methods of manufacturing LOKELMA, ensuring purity, yield, or specific crystalline forms.
- Method of Use Patents: These patents protect the use of LOKELMA for treating specific medical conditions, such as hyperkalemia. They can also cover specific dosing regimens or patient populations.
- Formulation Patents: Patents may exist for specific formulations of LOKELMA that offer advantages in terms of stability, delivery, or patient compliance.
Patent Term Extensions:
In many jurisdictions, including the United States (under the Hatch-Waxman Act) and Europe, patent terms can be extended to compensate for patent term lost during the regulatory review process. For LOKELMA, AstraZeneca would have sought these extensions to maximize its period of market exclusivity. The eligibility and duration of these extensions are dependent on specific country regulations and the timing of patent filings and approvals.
Regulatory Exclusivity:
Beyond patent protection, LOKELMA also benefits from regulatory exclusivity granted by regulatory authorities.
- New Chemical Entity (NCE) Exclusivity (US): In the US, a new drug that is not a biologic typically receives 5 years of NCE exclusivity from the date of approval. This prevents the FDA from accepting an ANDA (Abbreviated New Drug Application) for a generic version of the drug for the first four years. After four years, a generic company can file an ANDA, but the NCE exclusivity period remains a barrier for the first five years.
- Orphan Drug Exclusivity (if applicable): If LOKELMA was designated as an orphan drug for a rare disease indication, it could receive an additional 7 years of market exclusivity in the US and 10 years in the EU. However, hyperkalemia is not typically considered a rare disease.
- Data Exclusivity: Regulatory authorities grant periods of data exclusivity, during which generic manufacturers cannot rely on the innovator's clinical trial data to support their own applications. This period varies by region (e.g., 5 years for NCEs in the US, 8+2+1 years in Europe).
Generic Competition and Patent Challenges:
The exact expiry dates of key LOKELMA patents and the associated regulatory exclusivities are crucial for forecasting generic entry. Generic manufacturers often challenge innovator patents, leading to litigation. The outcomes of these legal battles can significantly impact the timeline for generic competition.
AstraZeneca actively monitors the patent landscape and defends its intellectual property. Investors and competitors closely track patent expiry dates and any legal challenges, as these are pivotal for understanding the long-term revenue potential and market dynamics of LOKELMA. Without specific patent numbers and expiry dates, which are often proprietary or complex to navigate, a precise timeline for generic entry cannot be provided here, but the strategy for protecting LOKELMA relies on both robust patent filings and leveraging available regulatory exclusivity periods.
What are the key risks and challenges facing LOKELMA?
LOKELMA, despite its established clinical profile and commercial momentum, faces several risks and challenges that could impact its market trajectory.
Key Risks and Challenges:
- Intensifying Competition: The hyperkalemia market is evolving. The emergence of new potassium binders or improved formulations of existing therapies can erode LOKELMA's market share. Competitors may also develop more cost-effective alternatives or therapies with superior efficacy or safety profiles in specific patient sub-groups.
- Payer Scrutiny and Pricing Pressures: As a specialty drug, LOKELMA is subject to rigorous scrutiny by payers (insurance companies, national health systems). Increasingly stringent reimbursement policies, formulary restrictions, and demands for greater evidence of cost-effectiveness can limit patient access and impact pricing power. This is particularly relevant in diverse global markets with varying healthcare funding models.
- Adherence and Patient Compliance: While LOKELMA offers dosing flexibility, long-term adherence can still be a challenge for patients managing chronic conditions. Factors such as the need for daily medication, potential side effects, and the complexity of managing multiple comorbidities can affect patient compliance, leading to suboptimal treatment outcomes and potentially impacting real-world effectiveness data.
- Adverse Event Profile: Although generally well-tolerated, LOKELMA can cause gastrointestinal side effects, including constipation and diarrhea. A higher-than-anticipated incidence or severity of these side effects in broader patient populations could lead to treatment discontinuation, impact physician prescribing patterns, and trigger additional safety monitoring requirements from regulatory bodies.
- Patent Expiry and Generic Entry: As LOKELMA's core patents approach expiry, the threat of generic competition increases. Generic alternatives, if approved, can significantly reduce market share and revenue due to lower pricing. The timing and impact of generic entry are subject to patent litigation and regulatory approvals.
- Regulatory Hurdles for Expansion: Expanding into new geographic markets involves navigating complex and varied regulatory approval processes. Delays in obtaining approvals, stringent data requirements, or different market access criteria in emerging economies can hinder global commercial expansion.
- Off-Label Use and Mismanagement: While LOKELMA is indicated for hyperkalemia, there is always a risk of off-label use or inappropriate prescribing, which could lead to adverse events or suboptimal outcomes. This can indirectly affect the drug's reputation and market perception.
- Healthcare Policy Changes: Broader shifts in healthcare policy, such as changes in drug pricing regulations, reimbursement frameworks, or drug approval processes, can create an unpredictable operating environment for pharmaceutical products like LOKELMA.
AstraZeneca's ongoing efforts in pharmacovigilance, market access negotiation, and lifecycle management are aimed at mitigating these risks. However, these challenges represent significant headwinds that require continuous strategic adaptation.
Key Takeaways
LOKELMA is a significant product in the hyperkalemia market, driven by its clinical advantages, including rapid onset and sustained efficacy. AstraZeneca's strategy for market expansion focuses on global launches, market access, and evidence generation, projecting continued revenue growth. The drug benefits from patent protection and regulatory exclusivity, but faces risks from intensifying competition, payer pressures, adherence challenges, and eventual generic entry.
FAQs
1. What are the primary indications for LOKELMA?
LOKELMA is indicated for the treatment of hyperkalemia in adult patients.
2. Does LOKELMA contain sodium?
LOKELMA contains minimal sodium. Its formulation is designed to be sodium-free for therapeutic purposes.
3. What is the typical duration of treatment with LOKELMA?
Treatment duration with LOKELMA varies depending on the patient's clinical condition, potassium levels, and response to therapy. It can be used for acute management and long-term maintenance.
4. Can LOKELMA be used in children?
As of current approvals, LOKELMA is indicated for adult patients. Pediatric use has not been broadly established or approved in major markets.
5. What is the mechanism of action for LOKELMA?
LOKELMA works by binding to potassium ions in the gastrointestinal tract, thereby reducing the amount of potassium absorbed into the bloodstream and promoting its excretion.
Citations
[1] A. M. Anker, M. W. D. Anker, H. E. Rupp, E. E. S. L. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. KD. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K. K