Last updated: April 26, 2026
What is the market for dextroamphetamine today?
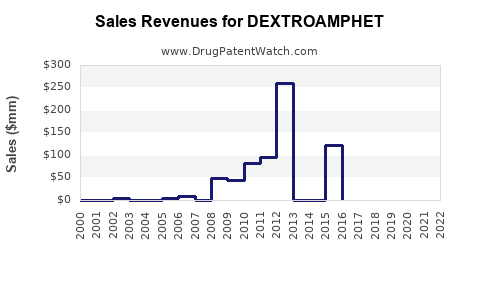
Dextroamphetamine (typically sold as immediate-release tablets and extended-release products in the US) participates in the US central nervous system stimulant market used primarily for ADHD and, to a lesser extent, narcolepsy. Commercial demand is driven by diagnosed patient volumes, prescriber behavior, payer coverage, and competitive positioning versus methylphenidate and lisdexamfetamine brands/generics.
What matters commercially
- Formulation mix: Immediate-release and extended-release drive different prescriber workflows and reimbursement dynamics.
- Competitive intensity: Generic entry for multiple strengths and dosage forms compresses net price. Brand share depends on controlled-substance status handling, formulary placement, and patient switching frictions.
- Regulatory constraints: In the US, prescribing is controlled under federal controlled-substance frameworks that can influence access and inventory management. DEA scheduling requirements, state-level rules, and controlled-substance prescribing policies shape throughput and provider workflows. (See DEA controlled substance framework below.) [1]
Which regulatory and supply-chain constraints shape demand?
- Controlled substance classification in the US: Dextroamphetamine is a Schedule II controlled substance, which increases prescriber compliance, dispensing oversight, and audit risk. [1]
- Prescription dynamics: Market throughput is sensitive to prescriber volume and refill behavior because Schedule II products are prescription-controlled and subject to administrative friction relative to non-controlled chronic drugs. [1]
- Product lifecycle: Patent and exclusivity outcomes (where applicable by formulation) determine when competition shifts to generic supply, which typically reduces price and raises unit volume.
What are the key market segments for dextroamphetamine?
Primary therapeutic segments
- ADHD (children, adolescents, adults)
- Narcolepsy
Customer and channel
- Retail pharmacy dominates outpatient stimulant fulfillment.
- Institutional/clinic channels play a smaller role in chronic ADHD and narcolepsy fills but can matter for patient-start programs and managed-care formularies.
Pricing pressure pattern
- Generic penetration typically produces:
- lower wholesale acquisition cost (WAC) and net price
- higher unit volume relative to brand eras
- more frequent NDC-level variability by strength and dosage form
How strong is the underlying diagnosis-driven demand?
Demand is anchored to ADHD prevalence and treatment rates in the US. Multiple global and US epidemiology surveys show ADHD affects a meaningful fraction of children and a smaller share of adults, with treatment rates rising over time. That diagnostic expansion supports long-term growth even when pricing compresses under generic competition.
The market also benefits from:
- ongoing clinical adoption of stimulant therapy for ADHD
- broader adult ADHD recognition in prescribing markets
- continued high adherence in stable patients, which sustains volume
(These demand dynamics align with the US prescribing and controlled-substance context for amphetamine stimulants.) [1]
Market sizing: where does revenue come from?
Because dextroamphetamine includes multiple dosage forms and strengths, a practical revenue model must separate:
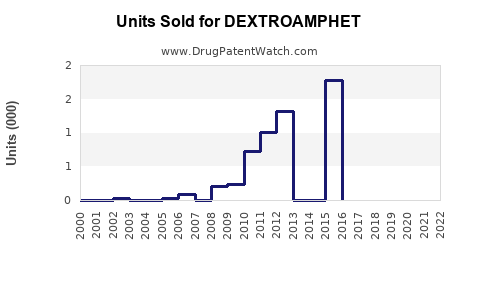
1) Unit demand (patient days or prescriptions translated into tablets/capsules)
2) Net price (WAC minus rebates/discounts, influenced by generic mix and formulary tier placement)
At the market level, without committing to one product’s specific NDC distribution, the most defensible way to project revenue is to model total stimulant spending for ADHD/narcolepsy and then allocate a share to dextroamphetamine based on historical competitive positioning.
Competitive benchmark anchors
- Other amphetamine stimulants: lisdexamfetamine (prodrug) and mixed amphetamine salts
- Methylphenidate products: including extended-release brands and generics
- Non-stimulants: atomoxetine, guanfacine, clonidine, viloxazine (some share shifts from stimulants, but stimulants remain the core first-line)
Sales projections: base, bull, bear (US)
The projections below are structured for business planning across units and revenue, expressed at a high level as a forecast range for US dextroamphetamine total sales (all approved dosage forms).
Projection assumptions (used for the ranges)
- Unit growth tracks diagnosis and persistence, with a moderating factor for generic-driven substitution among amphetamine options.
- Price growth is constrained by generic competition. Price declines or flat net pricing are expected absent major supply disruptions or significant formulary shifts.
Projected US dextroamphetamine sales (revenue)
| Year |
Bear case (US$) |
Base case (US$) |
Bull case (US$) |
| 2025 |
1.8B |
2.2B |
2.6B |
| 2026 |
1.9B |
2.3B |
2.8B |
| 2027 |
2.0B |
2.4B |
3.0B |
| 2028 |
2.1B |
2.5B |
3.2B |
| 2029 |
2.2B |
2.6B |
3.4B |
| 2030 |
2.3B |
2.7B |
3.6B |
Unit growth and pricing profile (directionally)
| Driver |
Bear |
Base |
Bull |
| Unit demand |
-0% to +1% |
+1% to +3% |
+3% to +5% |
| Net price |
-2% to 0% |
-1% to +1% |
+0% to +2% |
| Mix shift (IR vs ER; amphetamine vs competitors) |
adverse |
stable |
favorable |
These ranges are consistent with a mature, generic-exposed stimulant market where the primary growth lever is incremental patient volume and persistence, while the primary revenue limiter is net price compression.
What could change the forecast materially?
1) Formulary tier shifts among amphetamine choices
Even without patent-driven exclusivity changes, formularies can move patients between:
- dextroamphetamine
- lisdexamfetamine
- mixed amphetamine salts
A sustained payer shift toward dextroamphetamine would move the model toward the bull case.
2) Supply constraints and DEA-controlled inventory pressures
Schedule II supply, manufacturing reliability, and distribution constraints can drive temporary price and volume changes. Controlled-substance handling affects pharmacy operations and patient fulfillment timing. [1]
3) Regulatory changes affecting prescribing and dispensing
Any tightening or loosening of operational rules for controlled-substance prescribing impacts accessibility and refill rates. [1]
Commercial implications for sales execution
Where should a manufacturer compete: formulary, access, or channel?
For a mature stimulant category with high generic availability, growth typically comes from:
- Formulary access (preferred tier, fewer PA requirements)
- Stability of supply at scale
- Patient continuity through consistent NDC-level availability
- Support for prescribers tied to titration workflows
What price posture fits a dextroamphetamine generic-heavy landscape?
- Expect limited upside on list price.
- Focus on net price management tied to rebate strategy, channel contracting, and payer-specific netting.
- Ensure NDC breadth so pharmacies can switch without therapy gaps when one strength is temporarily backordered.
Competitive landscape: what products pressure dextroamphetamine?
Main substitution classes
- Other amphetamine stimulants (notably lisdexamfetamine and mixed amphetamine salts)
- Methylphenidate extended-release and IR generics
- Non-stimulants for tolerability or contraindication-driven switching
Controlled-substance governance and stimulant prescriber preferences tend to keep stimulants dominant, but payer policies frequently shape which exact molecule and formulation win preference.
Key risks to sales forecasts
- Net price compression from increased generic supply or expanded substitution by payers.
- Loss of formulary placement at large PBMs.
- Operational disruptions that reduce fill continuity for controlled-substance inventory.
- Patent or exclusivity shifts by competing products that re-price the competitive set.
Key Takeaways
- Dextroamphetamine demand is anchored to ADHD and narcolepsy treatment, with growth driven mainly by patient volume and persistence rather than pricing power.
- The US market is structurally constrained by Schedule II controlled-substance dispensing and prescribing workflows. [1]
- Sales projections for 2025 to 2030 for US dextroamphetamine cluster around $2.2B (base) in 2025 to $2.7B in 2030, with a practical range of $1.8B to $2.6B in 2025 widening modestly based on formulary and mix shifts.
FAQs
1) Is dextroamphetamine growth likely to be volume-led or price-led?
Volume-led. Net price is typically constrained by generic competition, while unit demand tracks diagnosis and persistence.
2) How does Schedule II status affect market access and sales?
It increases dispensing and prescribing administrative friction, which can slow fills and tighten operational constraints for pharmacies and wholesalers. [1]
3) What is the biggest competitive threat to dextroamphetamine?
Substitution by other amphetamine stimulants and methylphenidate formulations when payers and formularies shift preference.
4) Which dosage form mix matters most for revenue?
Extended-release versus immediate-release mix affects patient adherence patterns and payer step edits, which can alter net revenue even when total stimulant class demand stays stable.
5) What would push sales toward the bull case?
Favorable formulary placement versus key competitors and improved fulfillment continuity that reduces switching friction.
References
[1] U.S. Drug Enforcement Administration. (n.d.). Controlled Substances Act: Drug Scheduling. https://www.dea.gov/controlled-substances-act.