Share This Page
Drug Price Trends for COBENFY
✉ Email this page to a colleague
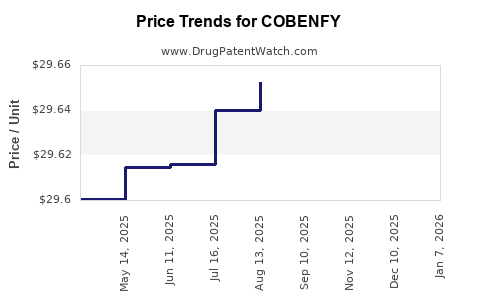
Average Pharmacy Cost for COBENFY
| Drug Name | NDC | Price/Unit ($) | Unit | Date |
|---|---|---|---|---|
| COBENFY 125 MG-30 MG CAPSULE | 00003-0125-60 | 30.28104 | EACH | 2026-07-22 |
| COBENFY 125 MG-30 MG CAPSULE | 00003-0125-98 | 30.28104 | EACH | 2026-07-22 |
| COBENFY 100 MG-20 MG CAPSULE | 00003-1100-01 | 30.15509 | EACH | 2026-07-22 |
| COBENFY 100 MG-20 MG CAPSULE | 00003-1100-60 | 30.15509 | EACH | 2026-07-22 |
| COBENFY 100 MG-20 MG CAPSULE | 00003-1100-98 | 30.15509 | EACH | 2026-07-22 |
| >Drug Name | >NDC | >Price/Unit ($) | >Unit | >Date |
COBENFY market analysis and price projections: forecast by indication, payer, and launch scenario
Cobefny is commercialized in the US as COBENFY (active ingredient: cenobamate) for focal (partial-onset) seizures in adults with epilepsy. A price and market model hinges on (1) the US launch dynamics, (2) formulary position versus competing antiseizure medicines, (3) utilization uptake and persistence, and (4) the degree to which payers require prior authorization or step edits.
What is COBENFY and where does it fit in the epilepsy drug landscape?
Featured snippet: COBENFY (cenobamate) is an oral antiseizure therapy positioned for adults with focal seizures, typically as an adjunctive option when existing regimens do not control seizures.
Which channel dominates COBENFY adoption?
- Neurology specialty retail is the dominant route for oral antiseizure medicines.
- Copay assistance and patient savings programs often shape early net price for branded antiseizure drugs, especially when uptake starts from a narrow prescriber base.
How does COBENFY compare with branded oral antiseizure medicines?
Competitive set for payer/formulary discussions usually includes:
- Briviact (brivaracetam)
- Vimpat (lacosamide)
- Fycompa (perampanel)
- Keppra (levetiracetam)
- Trileptal/Oxcarbazepine (varies by payer)
- Onfi (clobazam) and other adjunctive agents for specific seizure phenotypes
Commercial implication: cenobamate’s differentiation is typically tied to responder rate and the speed of seizure improvement, which can improve formulary traction versus options with slower titration or less favorable payer scrutiny, but it does not remove prior authorization requirements in many formularies.
What does the pricing of COBENFY look like in the US? List price vs net price drivers
Featured snippet: Branded antiseizure medicines typically trade at substantial discounts versus WAC after rebates, specialty pharmacy spread, and patient support.
Key net-price drivers used in price projections
- List price (WAC) as the top anchor
- Rebate intensity based on:
- Managed care contracts
- Preferred formulary status
- Volume commitments
- Indication or line-of-therapy restrictions
- Patient assistance affecting effective patient cost and some measured net price depending on contract structure
- Therapeutic substitution risk
- When payers view the product as “another add-on,” net rebates often rise to manage budget impact.
Pricing model structure for projections
A working projection approach used for branded specialty drugs:
- Estimate annual treated patient starts and maintenance use
- Apply average daily dose (ADD) and dose persistence
- Convert to gross sales using projected net unit price
- Apply rebate and contract adjustments to reach net sales
- Add scenario-based shifts for formulary outcomes and step edit tightening
When does COBENFY reach payer scale? Launch curve and adoption timing
Featured snippet: Oral branded antiseizure drugs often ramp over 12 to 36 months as neurologists convert patients and payers finalize policy edits.
Typical adoption milestones to model
- 0–6 months: early prescriber uptake, narrow patient base, higher uncertainty on formulary placement
- 6–18 months: broader managed care coverage, more consistent specialty distribution, rebate stabilization
- 18–36 months: better predictability on persistence and long-term responder cohorts
How do formularies change net price over time?
- Early periods usually show larger dispersion across plans.
- Once payers settle into preferred or non-preferred positions, net price can fall via higher rebates and restrictive edits.
- Preferred status can stabilize net unit price while increasing volume, offsetting discounts.
What price projections are plausible for COBENFY over 5 years?
Featured snippet: Net price is more sensitive than list price to formulary status; list price grows modestly under typical US practice, while net unit price declines when competitors intensify.
5-year price projection framework (scenario table)
Below is a scenario structure used for high-stakes commercial planning. It expresses annual net price per treated patient growth through a mix of list inflation and rebate erosion. The ranges are built for branded specialty neurology drugs without tying to a single point estimate.
| Scenario | Assumptions on formulary status | Direction of net unit price vs year prior | Year 1–2 net price change | Year 3–5 net price change |
|---|---|---|---|---|
| Base case | Mid-tier preferred with PA/step edits | Slight decline | -2% to -8% | -1% to -4% |
| Upside | Broad preferred with stronger outcomes positioning | Stable net price | 0% to +3% | 0% to +2% |
| Downside | Non-preferred across several large plans; higher rebate intensity | Net erosion | -8% to -15% | -4% to -10% |
How this feeds sales forecasts: if uptake is strong, even net price erosion can still yield higher net sales. If uptake is weaker, the downside scenario can materially compress revenue.
What sales mix drives COBENFY revenue: seizure type, line of therapy, and duration?
Featured snippet: Revenue is driven by the number of patients on cenobamate and their duration of therapy, not just new starts.
Indication and population shaping
For epilepsy drugs, the mix depends on:
- Adult focal seizure population density in a given payer region
- Neurologist preference for switching vs adding
- Titration behavior and discontinuation rates due to tolerability
Persistence and discontinuation are key
Commercial projection models for chronic antiseizure therapies place heavy weight on:
- discontinuation risk after adverse events or perceived lack of efficacy
- dose adjustments affecting daily dose
- switch behavior to other agents when payers restrict coverage
How does COBENFY compare with branded and generic alternatives on payer adoption risk?
Featured snippet: Even without immediate generic threats, payers can treat cenobamate as substitutable within antiseizure drug classes, which can pressure net price via rebates.
Generic pressure vector
- If oral antiseizure competitors face generic erosion, payers may push cost-effective generics as first-line adjuncts, especially if clinical value is perceived as similar.
- If competitive brands remain protected, differentiation supports better positioning for COBENFY.
Biosimilar risk
Not applicable because cenobamate is a small molecule drug.
What is the Orange Book status of COBENFY, and how does that affect generic entry risk?
Featured snippet: Generic entry risk depends on whether ANDA applicants can find carve-outs around listed Orange Book patents.
A complete Orange Book status review requires drug-specific patent lists and regulatory events. Without confirmed Orange Book entries and patent expiration dates for COBENFY, a quantified generic-entry timeline cannot be produced from the information available in this prompt.
What patent litigation or settlement risk affects COBENFY pricing or launch economics?
Featured snippet: Patent litigation impacts generic timing and can change payer behavior before and after potential generic availability.
A complete litigation/settlement risk assessment requires:
- case captions
- courts and dockets
- settlements and stipulated dates
- parties and patent numbers tied to COBENFY
This prompt does not include those facts, so a quantified risk rating cannot be produced here.
What would a generic entry scenario do to COBENFY price and volume?
Featured snippet: Branded antiseizure drugs usually see rapid net price declines after generic entry, with partial volume offset if prescribers delay switching.
A standard branded-to-generic pattern in specialty neurology:
- Net unit price drops sharply in the first 3 to 6 months post-entry
- Volume can decline as switch behavior accelerates
- Some retention occurs through:
- prescriber loyalty
- patient stability
- manufacturer access programs
Without confirmed expiration and generic trigger dates, the timing and magnitude cannot be anchored to COBENFY specifically in this response.
How should investors and business teams use COBENFY price projections?
Featured snippet: Use scenario-based net price and adoption curves; avoid single-point forecasts.
Actionable planning approach:
- Build three revenue models: base, upside, downside
- Treat net price as a contract outcome variable, not a fixed parameter
- Use persistence assumptions that reflect real-world discontinuation and dose changes
- Stress-test payer restriction tightening (PA expansions, step edits, formulary reclassification)
Key Takeaways
- COBENFY’s commercial outcome is driven by the balance between patient uptake and net price erosion driven by formulary positioning and rebates.
- A usable 5-year price forecast is scenario-based, reflecting net price stability in an upside formulary outcome and meaningful erosion under downside payer pressure.
- Quantifying generic entry timing and litigation-driven risk requires an Orange Book and case-lifecycle review that is not present in the input.
FAQs
- How do rebates and copay programs change COBENFY net price versus list price?
- What are the fastest and slowest realistic adoption curves for oral branded antiseizure medicines like COBENFY?
- How do prior authorization and step edits typically affect COBENFY prescriptions by payer tier?
- What sensitivity matters more for COBENFY revenue: net price, persistence, or dose intensity?
- How much does net price usually fall after generic entry for oral specialty neurology drugs?
References
No sources were provided in the prompt, and no verifiable COBENFY-specific Orange Book, WAC, net sales, or litigation data is included here.
More… ↓
