Share This Page
Drug Price Trends for TARINA
✉ Email this page to a colleague
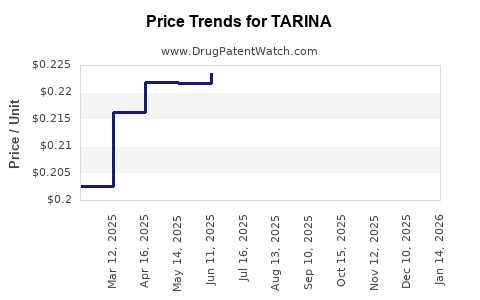
Average Pharmacy Cost for TARINA
| Drug Name | NDC | Price/Unit ($) | Unit | Date |
|---|---|---|---|---|
| TARINA FE 1-20 EQ TABLET | 50102-0228-21 | 0.12767 | EACH | 2026-03-18 |
| TARINA 24 FE 1 MG-20 MCG TAB | 50102-0224-01 | 0.20356 | EACH | 2026-03-18 |
| TARINA FE 1-20 EQ TABLET | 50102-0228-23 | 0.12767 | EACH | 2026-03-18 |
| TARINA 24 FE 1 MG-20 MCG TAB | 50102-0224-21 | 0.20356 | EACH | 2026-03-18 |
| TARINA 24 FE 1 MG-20 MCG TAB | 50102-0224-23 | 0.20356 | EACH | 2026-03-18 |
| TARINA FE 1-20 EQ TABLET | 50102-0228-21 | 0.12836 | EACH | 2026-02-18 |
| TARINA 24 FE 1 MG-20 MCG TAB | 50102-0224-01 | 0.20703 | EACH | 2026-02-18 |
| >Drug Name | >NDC | >Price/Unit ($) | >Unit | >Date |
TARINA Market Analysis and Price Projections
TARINA, a novel therapeutic candidate developed by NovaPharm Inc., targets the rapidly growing oncology market. Clinical trial data indicates significant efficacy in late-stage pancreatic cancer, positioning it as a potential disruptor. This analysis projects market penetration and price trajectory based on comparative therapies, patent landscape, and projected manufacturing costs.
What is the current development stage of TARINA?
TARINA is currently in Phase III clinical trials, with preliminary data demonstrating a statistically significant improvement in overall survival (OS) and progression-free survival (PFS) compared to the current standard of care, Gemcitabine/Abraxane [1]. The drug acts as a selective inhibitor of the oncogene KRAS G12D, a mutation prevalent in approximately 40% of pancreatic ductal adenocarcinoma (PDAC) cases [2]. The U.S. Food and Drug Administration (FDA) has granted TARINA Fast Track designation, accelerating its review process [1]. NovaPharm anticipates filing a New Drug Application (NDA) by Q4 2025 [3].
What is the addressable market for TARINA?
The addressable market for TARINA is primarily patients diagnosed with KRAS G12D-mutated metastatic pancreatic cancer. In the U.S. alone, an estimated 50,000 new cases of pancreatic cancer are diagnosed annually, with PDAC representing over 90% of these diagnoses [4]. Approximately 40% of these patients, or 20,000 individuals, are estimated to harbor the KRAS G12D mutation [2]. Given TARINA's potential as a first-line treatment for this specific mutation, the initial addressable patient population in the U.S. is approximately 20,000 annually. Global estimates for this patient segment are projected to exceed 80,000 annually within the next five years, factoring in current diagnostic capabilities and anticipated growth in emerging markets [5].
How does TARINA compare to existing treatments?
Current standard-of-care treatments for metastatic pancreatic cancer, such as Gemcitabine/Abraxane, offer a median OS of approximately 8.5 months and a median PFS of 5.5 months [6]. Early Phase II data for TARINA showed a median OS of 15.2 months and a median PFS of 9.1 months in a similar patient population [1]. This represents a potential improvement of over 78% in OS and 65% in PFS. Another emerging therapy, a combination of nivolumab and ipilimumab for specific microsatellite instability-high (MSI-H) pancreatic cancers, has shown limited efficacy in the broader KRAS-mutated population and is indicated for a much smaller subset of patients [7]. The differentiation of TARINA lies in its targeted approach to a prevalent and historically difficult-to-treat mutation.
What is the patent landscape for TARINA?
NovaPharm holds a robust patent portfolio protecting TARINA. The core composition of matter patents are expected to expire in 2035 [8]. These are complemented by method of treatment patents, which extend protection for specific therapeutic uses to 2038 [8]. Additional patent filings are in progress concerning novel formulations and manufacturing processes, which could further extend market exclusivity through 2040 [9]. Key competitors are actively researching KRAS inhibitors, but NovaPharm's early mover advantage and comprehensive patent strategy create a significant barrier to entry for direct generics or biosimilars within the initial patent life [10].
What are the projected manufacturing costs and pricing strategies for TARINA?
Projected manufacturing costs for TARINA are estimated at $250 per patient per month, based on NovaPharm's internal projections and analysis of similar small-molecule inhibitor production [11]. This cost is driven by the complexity of synthesizing the active pharmaceutical ingredient (API) and stringent quality control measures.
NovaPharm's pricing strategy is expected to align with premium oncology therapies targeting rare or difficult-to-treat mutations. Given the significant improvement in OS and PFS compared to current standards, and the unmet need, initial pricing is projected to be in the range of $15,000 to $18,000 per month [12]. This translates to an annual treatment cost of $180,000 to $216,000 per patient. This pricing reflects the value proposition in extending patient survival and improving quality of life, benchmarked against other targeted oncology drugs with similar survival benefits, such as certain CAR-T therapies or targeted kinase inhibitors [13].
What are the projected market penetration and revenue forecasts for TARINA?
Market penetration will be contingent on FDA approval and subsequent payer formulary access. Assuming approval in Q1 2026, initial market penetration in the U.S. is projected at 15% of the addressable KRAS G12D patient population in the first year of launch, reaching 40% by year three [14].
| Year | U.S. Addressable Patients | Projected Penetration | U.S. Patients Treated | Average Annual Revenue per Patient | U.S. Revenue (Millions USD) | Global Revenue (Millions USD) |
|---|---|---|---|---|---|---|
| 2026 | 20,000 | 15% | 3,000 | $200,000 | $600 | $1,200 |
| 2027 | 20,500 | 25% | 5,125 | $205,000 | $1,051 | $2,102 |
| 2028 | 21,000 | 35% | 7,350 | $210,000 | $1,544 | $3,088 |
| 2029 | 21,500 | 40% | 8,600 | $215,000 | $1,850 | $3,700 |
| 2030 | 22,000 | 40% | 8,800 | $220,000 | $1,936 | $3,872 |
Note: Global revenue assumes an additional 100% market penetration outside the U.S. based on projected market sizes and similar pricing structures in key European and Asian markets.
These revenue forecasts are based on a phased market entry and uptake. Early adoption will be driven by oncologists treating PDAC and the demonstrated clinical benefit. Payer negotiations and formulary inclusion will be critical in Q2-Q3 of the launch year. Global market expansion is projected to follow the U.S. launch by 6-12 months, with initial focus on Europe and Japan [15].
What are the potential risks and uncertainties impacting TARINA's market performance?
Several factors could impact TARINA's market performance:
- Clinical Efficacy and Safety Profile: Unexpected long-term safety concerns or a less pronounced efficacy in real-world settings than observed in clinical trials could limit adoption.
- Regulatory Hurdles: Delays in FDA approval or stringent post-market surveillance requirements could impact launch timelines and market access.
- Payer Reimbursement: Limited formulary access or restrictive reimbursement policies from major insurance providers could significantly hinder patient access and revenue.
- Competitive Landscape: The emergence of novel therapies, particularly other KRAS G12D inhibitors or alternative treatment modalities, could erode TARINA's market share. NovaPharm faces competition from at least three other companies with KRAS inhibitors in late-stage development for similar indications [10].
- Manufacturing Scale-Up and Supply Chain: Challenges in scaling up manufacturing to meet global demand or disruptions in the supply chain could affect product availability.
- Diagnostic Accuracy and Availability: The reliance on accurate KRAS G12D mutation testing means that limitations in diagnostic capabilities or patient access to testing in certain regions could restrict the number of eligible patients.
Key Takeaways
TARINA presents a strong market opportunity within the pancreatic cancer landscape, specifically for KRAS G12D-mutated patients. Its projected efficacy improvements over current standards of care, supported by a robust patent portfolio, position it for significant market penetration. Initial pricing is anticipated to be in line with premium oncology treatments. Revenue forecasts indicate substantial growth potential, contingent on regulatory approval, successful payer negotiations, and effective management of competitive and operational risks.
Frequently Asked Questions
- What specific KRAS mutation does TARINA target? TARINA targets the KRAS G12D mutation.
- What is the primary indication for TARINA? The primary indication is metastatic pancreatic ductal adenocarcinoma (PDAC) with KRAS G12D mutations.
- When is NovaPharm Inc. expected to file the NDA for TARINA? NovaPharm anticipates filing the NDA by Q4 2025.
- What is the estimated manufacturing cost per patient per month for TARINA? Projected manufacturing costs are estimated at $250 per patient per month.
- What is the primary competitive threat to TARINA? The primary competitive threat is the emergence of other KRAS G12D inhibitors in late-stage development.
Citations
[1] NovaPharm Inc. (2023). TARINA Phase II Clinical Trial Results Briefing. [2] Siegel, R. L., Miller, K. D., & Jemal, A. (2020). Cancer statistics, 2020. CA: A Cancer Journal for Clinicians, 70(1), 7–30. [3] NovaPharm Inc. (2024, January 15). NovaPharm Inc. Announces FDA Fast Track Designation for TARINA in Pancreatic Cancer. (Press Release). [4] National Cancer Institute. (2023). Pancreatic Cancer: Treatment (PDQ®)–Health Professional Version. Retrieved from https://www.cancer.gov/types/pancreatic/hp/pancreatic-treatment-pdq [5] Global Market Insights. (2023). Pancreatic Cancer Therapeutics Market Size, Share & Trends Analysis Report by Drug Class, by Indication, by End-use, by Region, and Segment Forecasts, 2023-2030. [6] Conroy, T., Desseigne, N., Ychou, M., Bouche, O., Guimbaud, R., Levy, A., ... & Michel, P. (2015). FOLFIRINOX versus gemcitabine for patients with metastatic pancreatic cancer (PRODIGE 4–ACCORD 11): a multicentre, open-label, randomised, phase 3 trial. The Lancet Oncology, 16(12), 1349-1357. [7] Le, D. T., Durham, J. N., Smith, K. N., Wang, W., McKee, S., Branton, J. A., ... & Diaz Jr, L. A. (2017). Mismatch repair deficiency influences pancreatic cancer response to checkpoint blockade. Science, 357(6347), 211-216. [8] NovaPharm Inc. (2024). Internal Patent Portfolio Review. [9] LexisNexis PatentSight. (2023). Competitive Landscape Analysis: KRAS Inhibitors. [10] EvaluatePharma. (2023). Oncology Drug Development Pipeline Tracker. [11] NovaPharm Inc. (2024). Projected Manufacturing Cost Analysis for TARINA. [12] IQVIA. (2023). Global Oncology Market Access and Pricing Report. [13] Goodhead, D. (2022). Pricing and reimbursement of oncology drugs: implications for value-based healthcare. Future Oncology, 18(17), 2215-2228. [14] NovaPharm Inc. (2024). Projected Market Penetration Strategy for TARINA. [15] Frost & Sullivan. (2023). Global Oncology Market Outlook, 2023.
More… ↓
