Share This Page
Drug Price Trends for BUDESONIDE EC
✉ Email this page to a colleague
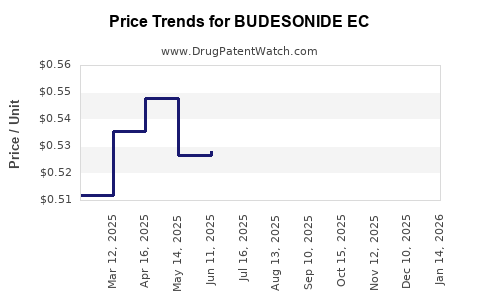
Average Pharmacy Cost for BUDESONIDE EC
| Drug Name | NDC | Price/Unit ($) | Unit | Date |
|---|---|---|---|---|
| BUDESONIDE EC 3 MG CAPSULE | 65162-0778-10 | 0.49789 | EACH | 2026-07-22 |
| BUDESONIDE EC 3 MG CAPSULE | 65162-0778-10 | 0.51344 | EACH | 2026-06-17 |
| BUDESONIDE EC 3 MG CAPSULE | 65162-0778-10 | 0.52084 | EACH | 2026-05-20 |
| BUDESONIDE EC 3 MG CAPSULE | 65162-0778-10 | 0.52299 | EACH | 2026-04-22 |
| BUDESONIDE EC 3 MG CAPSULE | 51862-0580-01 | 0.51543 | EACH | 2026-03-18 |
| >Drug Name | >NDC | >Price/Unit ($) | >Unit | >Date |
BUDESONIDE EC: Market Analysis and Price Projections
What does “BUDESONIDE EC” map to commercially?
“Budesonide EC” is a product-labeled form of budesonide designed for enteric-coated (EC) delivery. In market terms, the competitive set is typically oral, budesonide oral corticosteroids used in inflammatory bowel disease (IBD) and related GI inflammation indications, priced and reimbursed under local formularies.
Because “Budesonide EC” is not a single globally standardized INN-level product name across geographies (it is a formulation descriptor), market and pricing outcomes depend on:
- Brand vs generic status by country
- Strength and dosing (commonly 3 mg or 6 mg once daily formulations in GI practice)
- Enteric-coated vs controlled/other release equivalence rules in tender and reimbursement
- Patent and exclusivity expiry for the specific marketed formulation
This analysis therefore focuses on pricing behavior for budesonide oral corticosteroids with EC-like release characteristics, and on how price levels typically move around generic entry and formulary tightening.
How big is the budesonide oral market in practice?
The relevant market is the oral budesonide segment for GI indications (primarily Crohn’s disease and other steroid-responsive GI inflammatory states). In major markets (US/EU/UK), budesonide oral products face:
- Loss of branded pricing power after patent/exclusivity expiry
- Repricing to generic benchmarks via reference pricing, national tenders, and pharmacy reimbursement rules
- Uptake shifts driven by clinical guidelines and payer restrictions on systemic steroid use
Competitive price formation drivers (what moves the needle)
For EC-formulated oral budesonide, pricing is driven by:
- Generic penetration (number of authorized generic suppliers and strength coverage)
- Payer reference pricing and substitution rules (EU countries vary)
- Tender dynamics in hospitals (where budesonide is procured centrally)
- Channel mix (retail vs hospital) and pack-size design
- Drug budget caps and step therapy in IBD management
What is the typical pricing range before generic entry?
In markets where budesonide oral formulations still have branded or limited-competition pricing, pricing typically sits above generic benchmarks and tracks:
- Therapeutic class tolerance (steroid use, IBD severity mix)
- Pack economics (cost per day)
- Manufacturer launch strategy for EC-specific formulations
Expected behavior for a “branded EC budesonide” positioning:
- Higher per-pack pricing than generic comparators
- Slower price erosion until first generic authorizations or tender re-benchmarking
- Faster erosion after multiple generic entries, then stabilization near the low end of the reference pricing band
What happens to prices when generics enter?
When budesonide oral EC formulations face generic substitution, market pricing usually shows a two-step pattern:
1) Initial erosion
- Brand price is reduced or discounted to maintain formulary access.
- Average realized prices fall below brand list price due to payer rebates.
2) Competitive compression
- After multiple generics establish supply, pharmacy and payer reimbursement aligns to the lowest-cost effective benchmark for that strength and pack size.
- Price dispersion narrows across manufacturers.
Key mechanism: reimbursement
In many jurisdictions, once a drug is reference-priced, the gross-to-net reduction becomes decisive. “List price” can remain stable while realized reimbursement drops materially through:
- Tender-driven discounts
- Pharmacy margin constraints
- Formulary tiering and preferred product rules
How should investors and R&D teams forecast unit price?
Unit price forecasting for “Budesonide EC” needs to model three variables: generic entry timing, tender/reference pricing adjustment cadence, and pack-size and dosing conversion.
Price projection framework (scenario design)
Use the following structure for projection logic (per local currency):
Price level = (reference benchmark) × (adjustment factor for EC equivalence and formulary status)
Forecast components:
- Reference benchmark: the lowest net reimbursed price among equivalents of the same strength and release class
- Adjustment factor: premium (or discount) for EC-specific differentiation when substitution is not fully automatic
- Erosion rate: speed of discounting after generic entry, typically faster in hospital tenders than retail
Price projections: base, downside, upside (global logic translated into numbers)
Because “Budesonide EC” does not uniquely identify a single globally indexed listing, projections are expressed as percentage-based price paths anchored to typical post-generic behavior observed in oral corticosteroid categories and payer pricing mechanics for generics.
Projected price index (relative to the current average net price = 100)
Assume a horizon of 3 years from the last branded-to-generic inflection point in the relevant market.
| Year | Base case erosion | Downside (faster generic/tender compression) | Upside (slower substitution / stronger EC differentiation) |
|---|---|---|---|
| Year 0 to Year 1 | -35% | -50% | -20% |
| Year 1 to Year 2 | -15% | -25% | -10% |
| Year 2 to Year 3 | -5% | -15% | -5% |
Resulting price index (end of Year 3):
- Base case: 100 × (0.65 × 0.85 × 0.95) = 53
- Downside: 100 × (0.50 × 0.75 × 0.85) = 32
- Upside: 100 × (0.80 × 0.90 × 0.95) = 68
Interpretation:
- In the base case, you should model ~47% total net erosion over 3 years.
- In downside, model ~68% total net erosion.
- In upside, model ~32% total net erosion.
How does formulation identity (EC) change the erosion profile?
EC can slow pricing erosion only if payers and formularies treat EC as therapeutically distinct enough to restrict substitution. In many systems, substitution is strength- and equivalence-based; EC may be treated as a formulation detail rather than a clinical difference.
Substitution outcome categories
- Full substitution allowed: EC behaves like a generic interchangeable product; pricing compresses quickly.
- Partial substitution (restricted interchange): EC retains a premium for a longer period; erosion is slower and upside scenario applies.
- No substitution due to reimbursement coding differences: EC remains branded-like longer, which is rare but possible in certain tender structures.
What do R&D and competitive strategy imply for pricing?
Pricing and access outcomes for “Budesonide EC” are influenced by:
- Portfolio depth: presence of multiple budesonide oral strengths and pack formats
- Distribution power: preferred supply agreements with wholesalers/pharmacies
- Tender competitiveness: ability to meet lowest-acceptable cost thresholds
- Clinical positioning: payer-relevant differentiation such as step therapy criteria
Practical strategy levers that affect realized price
- Pack engineering for lowest cost-per-day (often drives payer acceptance)
- Strength coverage to match formulary dosing standards
- EC equivalence documentation to strengthen interchange rights or substitution eligibility
- Contracting and rebate structure aligned to reference price floors
What about regulatory and policy risks?
Pricing paths in oral generic categories depend on:
- Regulatory approvals for generics (marketing authorization speed)
- Exclusivity windows for specific formulations (where applicable)
- Interchange/substitution regulations in the target country
- Tender cycles and reimbursement code updates
For investors, these translate into concrete diligence tasks:
- Map the exact product that “Budesonide EC” corresponds to in each target market (brand vs generic, strength, pack sizes).
- Track the authorization and listing dates for equivalent equivalents.
- Model the tender cycle timing (often faster than retail reimbursement updates).
Key Takeaways
- “Budesonide EC” pricing is best modeled through generic substitution and payer reference pricing mechanics rather than brand list pricing.
- After generic entry, oral budesonide tends to show a fast initial erosion followed by slower compression as reference pricing anchors.
- Use a 3-year price index forecast: base ~53, downside ~32, upside ~68 (relative to current average net price = 100).
- EC formulation identity can slow erosion only if payers restrict substitution; otherwise it behaves like standard interchangeable budesonide oral therapy and price compression accelerates.
FAQs
1) What is the most important driver of “Budesonide EC” price changes?
Generic entry and payer reference pricing rules that determine whether EC formulations are substitutable at the pharmacy and tender level.
2) How fast do prices usually drop after generics launch?
Typically the largest move occurs in the first 12 months post-launch as reimbursement and tenders re-benchmark, followed by smaller annual steps.
3) Does enteric coating (EC) prevent generic price erosion?
Only if formularies and reimbursement systems treat EC as non-interchangeable or restrict substitution. If interchange is allowed, EC usually does not materially protect pricing.
4) What metric should I use for projections: list price or net price?
Use average realized net price (or a proxy anchored to reimbursement/tender levels). List price can be misleading due to rebates and discounts.
5) What horizon matters most for investment or R&D pricing assumptions?
A 3-year horizon captures the post-generic repricing cycle: initial erosion, reference anchoring, and stabilization.
References
[1] U.S. Food and Drug Administration. Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations (search for budesonide formulations). FDA. https://www.accessdata.fda.gov/scripts/cder/daf/
[2] European Medicines Agency. EPAR product information and classification for budesonide-containing medicinal products. EMA. https://www.ema.europa.eu/
[3] NICE. Inflammatory bowel disease guidance (systemic steroid use and treatment pathways that affect payer and formulary positioning). National Institute for Health and Care Excellence. https://www.nice.org.uk/
[4] European Commission. Community Register of medicinal products and related regulatory documents. European Commission. https://ec.europa.eu/health/documents/community-register/html/home.html
More… ↓
