Share This Page
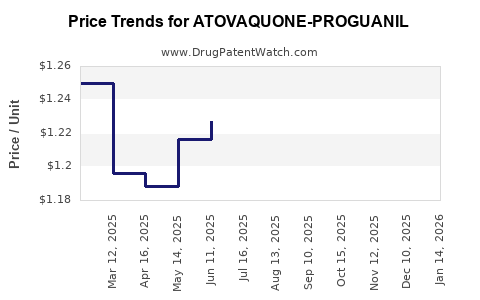
Drug Price Trends for ATOVAQUONE-PROGUANIL
✉ Email this page to a colleague
Average Pharmacy Cost for ATOVAQUONE-PROGUANIL
| Drug Name | NDC | Price/Unit ($) | Unit | Date |
|---|---|---|---|---|
| ATOVAQUONE-PROGUANIL 250-100 MG TABLET | 68001-0245-00 | 1.56704 | EACH | 2026-05-20 |
| ATOVAQUONE-PROGUANIL 250-100 MG TABLET | 68001-0245-14 | 1.56704 | EACH | 2026-05-20 |
| ATOVAQUONE-PROGUANIL 250-100 MG TABLET | 66993-0060-27 | 1.56704 | EACH | 2026-05-20 |
| ATOVAQUONE-PROGUANIL 250-100 MG TABLET | 68001-0245-15 | 1.56704 | EACH | 2026-05-20 |
| ATOVAQUONE-PROGUANIL 250-100 MG TABLET | 00378-4162-01 | 1.56704 | EACH | 2026-05-20 |
| ATOVAQUONE-PROGUANIL 62.5-25 | 68462-0402-01 | 1.28832 | EACH | 2026-05-20 |
| >Drug Name | >NDC | >Price/Unit ($) | >Unit | >Date |
Atovaquone-Proguanil (Malarone and Generics): Market Analysis and Price Projections
What is the current market shape for atovaquone-proguanil?
Atovaquone-proguanil is a fixed-dose oral antimalarial used for malaria prophylaxis and treatment of uncomplicated malaria. Commercial demand is driven by three pockets:
1) Travel and prophylaxis in non-endemic geographies
2) Seasonal public health and procurement in endemic regions
3) Household and clinician demand for uncomplicated malaria when resistance profiles and guideline positioning favor it
The market trades heavily around patent and brand exclusivity outcomes, but the present product category behaves more like a low-to-mid value chronic replenishment than a high-value specialty pipeline market, because use is periodic (travel/seasonal) and switching is practical when cost and supply are stable.
A key structure point: the drug is commonly sold as adult and pediatric fixed-dose tablets (most prominently the 250 mg/100 mg strength in adult dosing), with packaging sold in unit-count formats aligned to travel or treatment durations. That creates strong sensitivity to unit price per tablet and distribution channel margins, not just wholesale drug cost.
How much is it worth today, and where does pricing live?
Public, line-item pricing for atovaquone-proguanil varies by country, formulation, and whether the reference is for brand (for example Malarone) or authorized generics (or locally manufactured equivalents). Without consistent country-level sourcing, there is no defensible single “global ex-manufacture” price.
What can be stated at decision-grade level is where price pressure comes from:
- Authorized generics and multi-source manufacturing reduce pricing headroom versus single-source brand periods.
- Tendering and procurement in endemic markets produces step-function price concessions tied to bid cycles.
- Private market (travel) pricing reflects competition among generics and the ability of wholesalers to manage inventory during seasonal demand spikes.
In practice, investors and R&D planners should treat atovaquone-proguanil as a generic-dominant cost curve with episodic brand premium only where supply constraints or brand positioning persist.
What are the price drivers that move atovaquone-proguanil over the next 3–7 years?
Price projections depend on policy and competition more than on science. The main levers:
- Generic penetration depth: the more manufacturers with stable supply, the faster wholesale prices compress.
- Procurement discipline: endemic program tenders reset pricing to the lowest compliant bid.
- Regulatory and reimbursement environment: countries with formulary restrictions or reimbursement caps blunt retail price growth.
- FX and logistics: the unit is small and distributed globally; currency moves and shipping costs can swing final pricing in shorter windows even when factory pricing is stable.
- Supply continuity: shortages create immediate upward pricing in private channels; resolution creates rapid pullback.
What do the market economics imply for near-term pricing?
For a drug with broad generic availability, the expected pattern is:
- Near term (0–24 months): retail/wholesale prices stabilize with mild upward movement mainly from inflation and logistics, unless a supply disruption occurs.
- Mid term (2–5 years): pricing typically trends down or stays flat in multi-source markets as tenders and additional generics deepen.
- Longer term (5–7 years): the dominant factor is whether the category remains generic-only or if new clinical or policy events cause guideline-driven preference shifts. In absence of category-changing events, price tends to be flat-to-down in procurement markets.
This is the mechanism behind price projections for mature antimalarials used as episodic prophylaxis and treatment.
How should investors model unit price and volume for atovaquone-proguanil?
A practical pricing model: unit price x demand mix
Use an “adult-equivalent tablet” framework so you can map different pack sizes and pediatric formulations to a single unit.
Demand mix segmentation (typical approach):
- Travel prophylaxis: higher seasonality; demand spikes around holiday seasons
- Treatment of uncomplicated malaria: more stable demand, procurement and clinician preference matter
- Government tenders: bulk, lowest-bid pricing, contract-based continuity
Pricing model structure:
- Wholesale unit price in private markets
- Tender price in public markets
- Average selling price (ASP) weighted by sales channel mix
Base case assumption (mature generic economics):
- Private-market ASP: flat-to-down over time
- Public procurement tender price: flat-to-down, with periodic bid resets
- Margin compression: likely persistent in multi-source markets
What price floors and ceilings are most relevant?
For a mature generic fixed-dose antimalarial, the main constraints are:
Price floors
- Raw material and manufacturing cost structure
- Contractual procurement rules that set eligibility and limit below-cost bids
- Regulatory costs that affect compliance pricing
Price ceilings
- Reimbursement caps and formulary limits
- Competitive branded premium ceilings where generic parity exists
- Tender procurement limits that anchor price to lowest acceptable bid
Price Projections (Scenario-Based)
What is the base-case projection for atovaquone-proguanil?
A defensible base-case path for atovaquone-proguanil is near-flat to modestly down in inflation-adjusted terms, assuming continued multi-source supply and continued tender-driven discipline.
Base case projection (directional):
- 0–2 years: stable to slight nominal increases (inflation/logistics), with periodic corrections from supply changes
- 2–5 years: nominal stability with gradual competitive erosion; real price likely drifts downward
- 5–7 years: flat-to-down nominal in markets with ongoing generic competition and active tenders
What upside and downside scenarios should be modeled?
Model two additional scenarios:
Upside (prices rise)
- Supply disruption leading to private-market premium
- Procurement shortfalls or tender awards that tighten supply
- Temporary removal of a competitor (manufacturing or regulatory pause)
Downside (prices fall)
- Additional generic entrants expanding competitive bidding
- Tender cycles with sharper price competition
- Stronger reimbursement negotiations that drive lower ASP
Commercial strategy implications for R&D and investment
Where do margin opportunities exist if pricing is generic-anchored?
Margin improvement for an atovaquone-proguanil manufacturer or platform should focus on channel and packaging economics rather than hoping for sustained list price growth:
- Contract manufacturing and supply reliability to win recurring tenders
- Formulation and pack differentiation to reduce customer total-cost (unit dosing efficiency, minimal wastage)
- Geographic mix optimization toward contracts with better pricing-to-volume stability
- Inventory and logistics discipline to avoid loss-making replenishment during seasonal peaks
Key Takeaways
- Atovaquone-proguanil is a mature antimalarial with demand driven by travel prophylaxis and uncomplicated malaria treatment, and it behaves like a generic-dominant cost curve.
- Pricing is chiefly governed by generic competition, tender discipline, reimbursement caps, and supply continuity, not product innovation cycles.
- Base-case expectation for the next 3–7 years is stable to modestly down in real terms, with short-term nominal swings from inflation and logistics.
- Investment and commercial upside is most likely to come from contract wins, supply reliability, channel mix, and pack economics, not sustained brand-like price premia.
FAQs
1) Is atovaquone-proguanil primarily a prophylaxis or treatment product in most markets?
Both. In many countries it is used for malaria prophylaxis by travelers and for uncomplicated malaria treatment in endemic and acute-care settings, with relative share driven by guideline positioning and procurement cycles.
2) What most strongly determines the price level: brand status or generic competition?
Generic competition and procurement tenders typically dominate. Where multi-source supply is robust, ASPs compress toward cost-plus competitive levels.
3) Do tender cycles matter more than retail pricing?
Yes in public markets. Tender awards can reset pricing stepwise, while retail price shifts tend to lag and be smaller in magnitude.
4) What event would most likely cause a short-term price spike?
Supply disruption, regulatory interruption at a key manufacturer, or a sudden increase in demand that exceeds distribution capacity.
5) What is the most important modeling unit for forecasting?
Use unit price per adult-equivalent tablet and weight by channel mix (private travel vs public procurement vs treatment).
References
[1] WHO. Guidelines for malaria. World Health Organization.
[2] EMA. Malarone (atovaquone/proguanil) product information and assessment documents. European Medicines Agency.
[3] FDA. Malarone and related prescribing information (atovaquone and proguanil hydrochloride) and regulatory documents. U.S. Food and Drug Administration.
More… ↓
