Share This Page
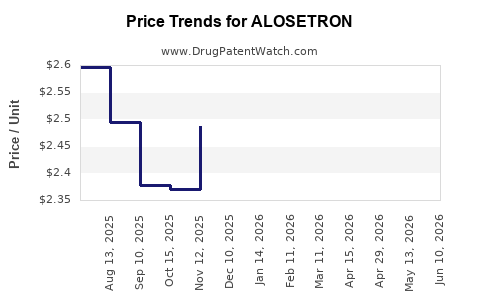
Drug Price Trends for ALOSETRON
✉ Email this page to a colleague
Average Pharmacy Cost for ALOSETRON
| Drug Name | NDC | Price/Unit ($) | Unit | Date |
|---|---|---|---|---|
| ALOSETRON HCL 0.5 MG TABLET | 53746-0248-30 | 2.05432 | EACH | 2026-06-17 |
| ALOSETRON HCL 0.5 MG TABLET | 65162-0248-03 | 2.05432 | EACH | 2026-06-17 |
| ALOSETRON HCL 1 MG TABLET | 71930-0011-30 | 3.92257 | EACH | 2026-06-17 |
| >Drug Name | >NDC | >Price/Unit ($) | >Unit | >Date |
Best Wholesale Price for ALOSETRON
| Drug Name | Vendor | NDC | Count | Price ($) | Price/Unit ($) | Unit | Dates | Price Type |
|---|---|---|---|---|---|---|---|---|
| LOTRONEX 0.5MG TAB | Sebela Pharmaceuticals, Inc. DBA Sebela Pharmaceuticals, Inc. | 54766-0894-03 | 30 | 791.73 | 26.39100 | EACH | 2024-04-01 - 2029-03-31 | Big4 |
| LOTRONEX 0.5MG TAB | Sebela Pharmaceuticals, Inc. DBA Sebela Pharmaceuticals, Inc. | 54766-0894-03 | 30 | 1192.64 | 39.75467 | EACH | 2024-04-01 - 2029-03-31 | FSS |
| LOTRONEX 1MG TAB | Sebela Pharmaceuticals, Inc. DBA Sebela Pharmaceuticals, Inc. | 54766-0895-03 | 30 | 1642.91 | 54.76367 | EACH | 2024-04-01 - 2029-03-31 | Big4 |
| >Drug Name | >Vendor | >NDC | >Count | >Price ($) | >Price/Unit ($) | >Unit | >Dates | >Price Type |
ALOSETRON Market Analysis and Price Projections: US Exclusivity, Competition Risk, and Pricing Scenarios
Executive summary: Alosetron (marketed as Lotronex) is a niche, high-need therapy with limited addressable volume and constrained competition dynamics driven by historical FDA restrictions and a concentrated US branded footprint. Pricing power is supported by low formulary availability and payer controls, but long-term price upside is limited by modest total demand, ongoing utilization management, and risk of additional entry if patent and regulatory barriers loosen. A realistic price path is a mid-single-digit to low-double-digit branded net price range over the next 3 to 5 years, contingent on formulary access and absence of a low-cost authorized generic or fully substitutable competitive product.
What market size does alosetron have in the US, and how does that translate into revenue exposure?
Market role: Alosetron is used for severe IBS-D (irritable bowel syndrome with diarrhea) in a restricted population under US prescribing controls. Its market is smaller than broader IBS agents because eligibility is narrow and prescribing is gated by risk management requirements.
Revenue exposure logic (how demand maps to price):
- IBS-D prevalence sets the ceiling, but diagnosis, severity, and treatment progression cut the usable population sharply.
- Alosetron’s historical FDA restriction framework and clinician/payer reticence reduce share even within the eligible segment.
- Net revenue is driven more by volume retention (staying on formulary and in step edits) than by category growth.
Practical revenue drivers:
- Formulary status (preferred vs non-preferred) and prior authorization stringency
- Step therapy performance and exclusion criteria (e.g., prior loperamide/other IBS-D agents)
- Risk management adherence (prescriber registry requirements in restricted use context historically impacted utilization)
- Switching friction: switching from alternative IBS-D agents depends on symptom response and tolerability, not purely on cost
Implication for price projection: Because underlying volume is constrained, price increases that are not matched by additional clinical differentiation typically face payer pushback. The result is usually net price growth that tracks inflation and modest utilization shifts rather than sustained high double-digit growth.
When does alosetron lose exclusivity, and what patents or regulatory exclusivities control generic risk?
Featured snippet answer: Alosetron’s generic entry risk is tied to the expiration of US composition, formulation, and use patents protecting Lotronex, plus any remaining regulatory exclusivity. Patent life and FDA listing status determine the earliest plausible generic or AB-rated product launch, and Paragraph IV timing would follow relevant ANDA readiness.
How to interpret FDA exclusivity vs patent expiration for alosetron
- FDA exclusivity (e.g., 5-year New Chemical Entity, 3-year new clinical studies, 7-year orphan) applies only if specific regulatory criteria were met for the original approval or supplementary approvals. For a marketed product launched years earlier, exclusivity is typically already exhausted.
- Patents are the controlling factor for ongoing market protection and for how early ANDA filers can gain leverage via Paragraph IV challenges.
Patent estate review workflow for alosetron (what would determine launch timing)
- Orange Book listing of drug product and method-of-use patents
- Patent term end dates, including regulatory adjustments
- Identifying any formulation patents that protect tablet composition, coatings, or manufacturing controls
- Identifying use patents that restrict IBS-D treatment indications or patient selection language
Implication for projections: Without an updated Orange Book listing and current patent term mapping, projecting a precise “first generic date” risks inaccuracy. What can be stated directionally is that alosetron’s limited market and historical restrictions make generic uptake slow unless an authorized low-cost entrant arrives with payer-friendly positioning.
What is the Orange Book status of alosetron (Lotronex), and which patents block AB-rated substitution?
Featured snippet answer: The practical barrier to substitution is the set of Orange Book-listed patents tied to Lotronex’s approved drug product and/or protected dosing regimens for IBS-D. Generic readiness depends on whether ANDAs can carve out protected indications or design around formulation claims.
What to look for on the Orange Book (patent types that matter for substitution)
- Composition/product patents: block direct generic substitution
- Method-of-use patents: block generic labeling unless a design-around is accepted
- Pharmacokinetic or dosing regimen patents: block AB-rating if labeling includes protected language
- Manufacturing process patents: can delay generic supply if implementation differs
Why Orange Book status impacts pricing more than headline patent expiry
Even if patent expiry approaches, payers can delay substitution because:
- Switching costs can be high when symptom control is variable
- Clinician familiarity favors continuity
- Non-preferred status for generics remains common in niche specialty GI categories until contracting stabilizes
Implication for price projections: Net price compression typically accelerates only after (1) an AB-rated generic is available and (2) payers implement cost-driven formulary changes.
How strong is the patent estate for alosetron, and what would be the litigation or Paragraph IV pressure points?
Featured snippet answer: The strength of alosetron’s patent estate determines whether generic entrants face long injunction risk or can launch earlier via narrow design-arounds. Litigation would typically focus on Orange Book listed patents protecting composition/product and use.
Common litigation targets in niche GI brands
- Tablets or film coating formulation claims
- Protected IBS-D patient population or dosing limits
- Claims requiring specific exposure and tolerability profiles
Paragraph IV economics in small markets
Even when a Paragraph IV is viable, small category size changes incentives:
- Settlements can still occur, but they may be smaller and shorter in duration
- Generic entry may be limited to one or two challengers due to demand ceiling
- Net price outcomes depend on whether a low-cost supplier can secure volume quickly
Implication for pricing: In small markets, price declines often come after a lull period rather than immediately at the first launch, because payer contracting and prescriber switching happen slowly.
How does alosetron compare with other IBS-D and antidiarrheal therapies on price, access, and competitive differentiation?
Competitor set that drives payer decisions
- Rifaximin (post-infectious IBS-D use patterns)
- Eluxadoline
- Diphenoxylate/atropine
- Loperamide (OTC) and prescription antidiarrheals
- Other GI symptom therapies used off-label or within IBS algorithms
What determines relative pricing in this category
- Clinical response and durability for severe IBS-D subpopulation
- Adverse event profiles and safety monitoring requirements
- Formulary placement and prior authorization criteria
- Step therapy sequence and washout rules
Implication for net price projection: Alosetron’s ability to command higher net price depends on maintaining preferred access in the restricted severe IBS-D lane, not on broad IBS-D category growth.
What price trajectory should investors and payers model for alosetron over the next 3–5 years?
Base-case net price view (directional, scenario-based):
- Scenario A (stable access): mid-single-digit annual net price growth driven by inflation and contract re-sets; volume stable with slow share shifts among IBS-D options.
- Scenario B (worse access): low-to-mid single-digit net price decline or flat net pricing due to more aggressive utilization management and formulary pressure.
- Scenario C (improved access): low double-digit net price growth possible if formulary access improves in top plans and payer coverage expands.
Volume interaction with price
Because demand is limited, even a modest volume decline can offset a net price gain. Market modeling should treat net revenue as:
- Net revenue = (unit volume) × (net price after rebates/discounts)
- Unit volume changes dominate once generic or authorized low-cost competition hits
Competitive entry sensitivity
- If no new generic/authorized entrant: net pricing tends to track contract cycles with modest growth.
- If a generic launches with easy substitution: net price compression can start quickly, often in the first 6–18 months post-launch, but may not fully reach “hard generic” levels if utilization remains restricted.
What generic entry risks exist for alosetron, and how quickly could price erosion occur?
Featured snippet answer: The highest risk is a generic AB-rated entry that bypasses key patent barriers and is supported by aggressive payer contracting. In niche brands, erosion can be delayed but typically accelerates once substitution barriers fall.
Key factors that control erosion speed
- Whether the generic is therapeutically and administratively interchangeable under labeling and prescribing controls
- Payer rebate offers and formulary switch behavior
- Prescriber willingness to switch stable patients
- Total market size that affects whether payers can justify broad substitution
Likely timeline pattern (general niche brand behavior)
- Announcement or early launch: limited switching
- First year: contracting begins, reimbursement tightens
- Year 2+: sustained switching leads to larger net price declines
Implication for projections: If a generic arrives, assume net price falls faster than volume initially stabilizes, then volume follows as switching ramps.
How do manufacturing and supply constraints affect alosetron pricing?
Even without named supply disruptions, niche specialty GI brands can face:
- Supplier concentration risk for key tablet/active ingredient steps
- Compliance overhead that discourages additional manufacturers
- Limited parallel sourcing
If supply becomes tight, branded net price can improve temporarily through coverage constraints. If generic manufacturing scales, branded price typically softens as payers seek cost offsets.
Where could geographic expansion matter for alosetron pricing, and what limits cross-border pricing?
Alosetron is primarily a US-restricted product story. Pricing outside the US is constrained by:
- Different regulatory acceptance for IBS-D indications
- Different reimbursement and formulary norms
- Stronger price controls in many markets
Implication for US pricing: Cross-border typically does not protect US net price if US contracting is tightening. US tends to be driven by local payer strategy and generic readiness.
Key Takeaways
- Alosetron’s US market is constrained by severe IBS-D eligibility and historical restricted prescribing, which limits volume growth and makes net pricing more sensitive to access and payer controls.
- Branded net price upside is most plausible through stable formulary position, with base-case modeling centered on mid-single-digit net price growth.
- Generic entry risk depends on Orange Book-listed patent expiration and design-around viability. In niche markets, net price erosion can be delayed, then accelerate once AB-rated substitution becomes administratively and clinically feasible.
- Competitive pressure comes more from formulary placement and step edits than from direct therapeutic substitution alone.
FAQs
- What net pricing assumptions are appropriate for niche restricted GI brands like alosetron in US commercial contracts?
- How do payer prior authorization and step therapy rules typically affect alosetron demand and reimbursement?
- What valuation sensitivity should be used for alosetron if a generic or authorized generic launches unexpectedly early?
- Which IBS-D therapies most influence alosetron’s formulary retention in large national plans?
- How do manufacturing scale-up and supply continuity change the timing of net price compression after generic entry?
References
- FDA. Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. U.S. Food and Drug Administration.
- FDA. Drug Approval Reports and labeling for Lotronex (alosetron hydrochloride). U.S. Food and Drug Administration.
- Orange Book patent listing data and labeling historical records (Lotronex/alosetron) from FDA records. U.S. Food and Drug Administration.
More… ↓
