EMTRIVA Drug Patent Profile
✉ Email this page to a colleague
When do Emtriva patents expire, and what generic alternatives are available?
Emtriva is a drug marketed by Gilead and is included in two NDAs.
The generic ingredient in EMTRIVA is emtricitabine. There are eighteen drug master file entries for this compound. Three suppliers are listed for this compound. Additional details are available on the emtricitabine profile page.
DrugPatentWatch® Litigation and Generic Entry Outlook for Emtriva
A generic version of EMTRIVA was approved as emtricitabine by CIPLA on July 2nd, 2018.
AI Deep Research
Questions you can ask:
- What is the 5 year forecast for EMTRIVA?
- What are the global sales for EMTRIVA?
- What is Average Wholesale Price for EMTRIVA?
Summary for EMTRIVA
| US Patents: | 0 |
| Applicants: | 1 |
| NDAs: | 2 |
| Finished Product Suppliers / Packagers: | 1 |
| Raw Ingredient (Bulk) Api Vendors: | 119 |
| Clinical Trials: | 13 |
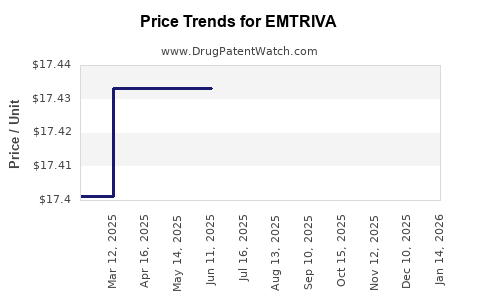
| Drug Prices: | Drug price information for EMTRIVA |
| Patent Litigation and PTAB cases: | See patent lawsuits and PTAB cases for EMTRIVA |
| What excipients (inactive ingredients) are in EMTRIVA? | EMTRIVA excipients list |
| DailyMed Link: | EMTRIVA at DailyMed |

Paragraph IV (Patent) Challenges for EMTRIVA
| Tradename | Dosage | Ingredient | Strength | NDA | ANDAs Submitted | Submissiondate |
|---|---|---|---|---|---|---|
| EMTRIVA | Capsules | emtricitabine | 200 mg | 021500 | 1 | 2012-07-16 |
US Patents and Regulatory Information for EMTRIVA
| Applicant | Tradename | Generic Name | Dosage | NDA | Approval Date | TE | Type | RLD | RS | Patent No. | Patent Expiration | Product | Substance | Delist Req. | Exclusivity Expiration |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gilead | EMTRIVA | emtricitabine | CAPSULE;ORAL | 021500-001 | Jul 2, 2003 | AB | RX | Yes | Yes | ⤷ Start Trial | ⤷ Start Trial | ⤷ Start Trial | |||
| Gilead | EMTRIVA | emtricitabine | SOLUTION;ORAL | 021896-001 | Sep 28, 2005 | RX | Yes | Yes | ⤷ Start Trial | ⤷ Start Trial | ⤷ Start Trial | ||||
| >Applicant | >Tradename | >Generic Name | >Dosage | >NDA | >Approval Date | >TE | >Type | >RLD | >RS | >Patent No. | >Patent Expiration | >Product | >Substance | >Delist Req. | >Exclusivity Expiration |
EU/EMA Drug Approvals for EMTRIVA
| Company | Drugname | Inn | Product Number / Indication | Status | Generic | Biosimilar | Orphan | Marketing Authorisation | Marketing Refusal |
|---|---|---|---|---|---|---|---|---|---|
| Gilead Sciences Ireland UC | Emtriva | emtricitabine | EMEA/H/C/000533Emtriva is indicated for the treatment of HIV-1 infected adults and children in combination with other antiretroviral agents.This indication is based on studies in treatment-naive patients and treatment-experienced patients with stable virological control. There is no experience of the use of Emtriva in patients who are failing their current regimen or who have failed multiple regimens.When deciding on a new regimen for patients who have failed an antiretroviral regimen, careful consideration should be given to the patterns of mutations associated with different medicinal products and the treatment history of the individual patient. Where available, resistance testing may be appropriate. | Authorised | no | no | no | 2003-10-24 | |
| >Company | >Drugname | >Inn | >Product Number / Indication | >Status | >Generic | >Biosimilar | >Orphan | >Marketing Authorisation | >Marketing Refusal |
International Patents for EMTRIVA
See the table below for patents covering EMTRIVA around the world.
| Country | Patent Number | Title | Estimated Expiration |
|---|---|---|---|
| Ireland | 920545 | ⤷ Start Trial | |
| Luxembourg | 91073 | ⤷ Start Trial | |
| China | 1084745 | ⤷ Start Trial | |
| Australia | 2006207874 | ⤷ Start Trial | |
| Japan | 3530150 | ⤷ Start Trial | |
| Norway | 324979 | ⤷ Start Trial | |
| >Country | >Patent Number | >Title | >Estimated Expiration |
Supplementary Protection Certificates for EMTRIVA
| Patent Number | Supplementary Protection Certificate | SPC Country | SPC Expiration | SPC Description |
|---|---|---|---|---|
| 0915894 | 08C0020 | France | ⤷ Start Trial | PRODUCT NAME: EFAVIRENZ; EMTRICITABINE; TENOFOVIR DISOPROXIL FUMARATE; REGISTRATION NO/DATE: EU/1/07/430/001 20071213 |
| 1632232 | SPC/GB17/008 | United Kingdom | ⤷ Start Trial | PRODUCT NAME: A COMBINATION OF RILPIVIRINE HYDROCHLORIDE, EMTRICITABINE, AND TENOFOVIR ALAFENAMIDE, OR A PHARMACEUTICALLY ACCEPTABLE SALT THEREOF, IN PARTICULAR TENOFOVIR ALAFENAMIDE FUMARATE.; REGISTERED: UK EU/1/16/1112 (NI) 20160623; UK PLGB 11972/0019 20160623 |
| 0582455 | 08C0021 | France | ⤷ Start Trial | PRODUCT NAME: EFAVIRENZ; EMTRICITABINE; TENOFOVIR DISOPROXIL FUMARATE; REGISTRATION NO/DATE: EU/1/07/430/001 20071213 |
| 1663240 | 1590057-4 | Sweden | ⤷ Start Trial | PRODUCT NAME: A COMBINATION OF RILPIVIRINE, OR A PHARMACEUTICAL LY ACCEPTABLE SALT OF RILPIVIRINE, INCLUDING THE HYDROCHLORIDE SALT OF RILPIVIRINE, AND TENOFOVIR DISOPROXIL, IN PARTICULAR TENOFOVIR DISOPROXIL FUMARATE, AND EMTRICITABINE; REG. NO/DATE: EU/1/11/737 20111128 |
| 1663240 | 92855 | Luxembourg | ⤷ Start Trial | PRODUCT NAME: COMBINAISON DE RILPIVIRINE OU UNE FORME THERAPEUTIQUE EQUIVALENTE QUI EN DERIVE TELLE QUE PROTEGEE PAR LE BREVET DE BASE, TEL QU'UN SEL PHARMACEUTIQUEMENT ACCEPTABLE DE RILPIVIRINE, INCLUANT LE SEL CHLORHYDRATE DE RILPIVIRINE , TENOFOVIR, EN PARTICULIER LE FUMARATE DE TENOFOVIR DISOPROXIL, ET L'EMTRICITABINE. |
| 3808743 | 2290034-4 | Sweden | ⤷ Start Trial | PRODUCT NAME: A COMBINATION OF RILPIVRINE OR A THERAPEUTICALLY EQIVALENT FORM THEREOF PROTECTED BY THE BASIC PATENT, SUCH AS A PHARMACEUTICALLY ACCEPTABLE ADDITION SALT OF RILPIVIRINE, INCLUDING THE HYDROCHLORIC ACID SALT OF RILPIVIRINE, AND EMTRICITABINE; REG. NO/DATE: EU/1/11/737/001-002 20111128 |
| >Patent Number | >Supplementary Protection Certificate | >SPC Country | >SPC Expiration | >SPC Description |
EMTRIVA (emtricitabine) market dynamics and financial trajectory: revenue drivers, pricing, exclusivity cliffs, and generic pressure
More… ↓
Make Better Decisions: Try a trial or see plans & pricing
Drugs may be covered by multiple patents or regulatory protections. All trademarks and applicant names are the property of their respective owners or licensors. Although great care is taken in the proper and correct provision of this service, thinkBiotech LLC does not accept any responsibility for possible consequences of errors or omissions in the provided data. The data presented herein is for information purposes only. There is no warranty that the data contained herein is error free. We do not provide individual investment advice. This service is not registered with any financial regulatory agency. The information we publish is educational only and based on our opinions plus our models. By using DrugPatentWatch you acknowledge that we do not provide personalized recommendations or advice. thinkBiotech performs no independent verification of facts as provided by public sources nor are attempts made to provide legal or investing advice. Any reliance on data provided herein is done solely at the discretion of the user. Users of this service are advised to seek professional advice and independent confirmation before considering acting on any of the provided information. thinkBiotech LLC reserves the right to amend, extend or withdraw any part or all of the offered service without notice.
ISSN: 2162-2639

Privacy and Cookies
Terms & Conditions
Site Map
DrugPatentWatch Alternatives
LOE / Major Patent Expirations 2026 - 2027
NCE-1 Patent Challenge Dates 2026 - 2027
Friedman, Yali. "DrugPatentWatch" DrugPatentWatch, thinkBiotech, 2026, www.DrugPatentWatch.com.
See Primary Research Papers Citing DrugPatentWatch